Click for SiteMap
sociology:epidemiology
change site colors:
Table of Contents
The motive for this article is to expose the lack of consideration for alternate accounts on the severity or progression of the COVID pandemic, to combat mass groupthink that has consistently plagued society throughout history.
For example, pollution is responsible for the deaths of more people than COVID will ever kill, but humanity will not choose to slow manufacturing and try to be satisfied with less money, war, or empirialism that would eventually save billions of people. There is a complete lack of objectivity with regards to the larger picture. While an important topic on its own, the pandemic has become a fashionable topic with which countries and politicians must save face due to media influence in public opinion.
Yet even within the topic of the pandemic itself, misinformation takes a life of its own due to the accumulation of political and capitalist motivations and mass fear of something novel.
History of Pandemics

Terminology
Case Fatality Rate: number of deaths compared to / the number of those that are known to have been infected.
Infection Fatality Rate: number of deaths compared to / the number of those that are estimated to have been infected.
Crude Mortality Rate: number of deaths from all-causes compared to / the number of the entire population
Coronavirus COVID-19 Pandemic 2020
MONTY PYTHON HUMOR WITHIN. DON'T PANIC. STAY CALM AND CARRY ON.
Older dated entries are still relevant, and have been updated.
Projected Crude Mortality Rate, deaths from all causes globally per year, is estimated as having increased by 0.020%, due to SARS-CoV-2.
Update 20201220: that figure is now approximately .04% (7.7 billion * 0.04 = 3.8 million)
Progression of the Pandemic by Region:

USA Crude Mortality Rate, showing an excess due to COVID-19:

May 20 2022
A New World Health Organization Report Once Again Proves Sweden Right, Ian Miller
How Sweden's COVID Gamble Paid Off, dailymail.co.uk
Pandemics have always been measured by excess deaths. Is excess deaths the most accurate measure of a pandemic? It may not be perfect, but it's what epidemiologists go by.
September 30 2021
A vaccine for new variants should have come out a long long time ago. Please don't make excuses.
https://www.vox.com/future-perfect/22687728/delta-specific-booster-vaccine-covid
Pharma probably decided they could still sell the old vaccine, without spending additional on R&D to create new variant specific vaccines.
May 19, 2021
Countries with High Vaccination Rates Continue with COVID-19 Epidemics
What's this all about? All vaccinated, but looks like the variants have taken over in Seychelles. Need to find out what vaccine they used:
https://www.bloomberg.com/news/articles/2021-05-04/world-s-most-vaccinated-nation-reintroduces-curbs-as-cases-surge
Also in Maldives:
https://maldives-stays.com/blog/128
Update 20210529:
Sorting countries by percentage of people with at least one vaccination dose, it isn't unanimous that the vaccines make the pandemic disappear:

The following countries are among the highest in vaccination rates, yet still have a COVID-19 epidemic (based on worldometer charts):
Seychelles 72%, Bhutan 63%, Maldives 57%, Mongolia 56%, Canada 55%, Chile 54%, Bahrain 53%, United Arab Emirates 51%, Uruguay 50%, Qatar 49%.
In each country, what vaccines did they administer, and what variants are prevalent? There are people getting vaccinated with the old variant vaccines, when the new variant is prevalent. It would be negligent to be giving a non-updated vaccine. One of them is tied up in red tape: NIH clinical trial evaluating Moderna COVID-19 variant vaccine begins, nih.gov 20210331.
Update 20210801:
Seychelles, Bhutan, Mongolia, and United Arab Emirates are now having lower case rates, although still substantial. The rest of the countries mentioned earlier have mostly resolved their covid epidemics. I don't know if because of vaccinations or because of natural herd immunity.
Countries Without Vaccinations Show Pandemic Remission
Meanwhile, there are countries that are clear of their epidemic, which have had no vaccines, such as (not all-inclusive):





Notice that I am using cases data, because for smaller countries there are too few deaths to make a good plot curve.
Gibraltar Finishes Vaccinations

Feb 28, 2021
The World Could Have Used A Patent-Free Vaccine in June
“Back in the spring, I still thought that surely some public entity will get involved and start pushing it forward. Turns out that no situation is urgent enough to compel the state to start actively pursuing something like this.”
The research team includes some of Finland’s scientific heavyweights, such as Academy professor Seppo Ylä-Herttuala of the A. I. Virtanen Institute, a former president of the European Society of Gene and Cell Therapy, and academician Kari Alitalo, a foreign associated member of the National Academy of Sciences in the United States. They believe their nasal spray, built on well-established technology and know-how, is safe and highly effective.
“It’s a finished product, in the sense that the formulation will no longer change in any way with further testing,” Saksela says. “With what we have, we could inoculate the whole population of Finland tomorrow.”
But instead of exploring the potential of intellectual property–free research, Finland, like other Western countries, has continued to follow the default policy of the last several decades: to lean fully on Big Pharma.
The Finnish vaccine provides a striking case study of the many ways in which the contemporary patent-based funding model has slowed down vaccine development. Finland Had a Patent-Free COVID-19 Vaccine Nine Months Ago — But Still Went With Big Pharma, jacobinmag 20210228
“In the mainstream narrative, the first-generation COVID-19 vaccines from Pfizer, Moderna, and AstraZeneca are typically presented as an illustration of how markets incentivize and accelerate vital innovation. In reality, the fact that the profit motive is the overriding force shaping medical research has been devastating.” The profit-stoking patent protection which governments lavish on corporations, even during a global pandemic, “is especially absurd when we consider that so-called private pharmaceutical research is itself majority public funded. . . .
“In other words, we are paying for the same shot twice: first for its development, then for the finished product. But there might be even a third price tag, since governments have agreed to assume responsibility for the potential side effects of coronavirus shots. This is a typical dynamic between large corporations and states: profits are private, risks are socialized. . . . “The damage goes well beyond shortages and high prices. For one, stopping a disease in its tracks is bad business. ”
Finland had a patent-free nasal spray COVID-19 vaccine, which they called “the Linux of vaccines,” since May 2020. It was never developed or distributed, because the python of pharma has a death grip on our world. - commentary by Annie Gottlieb
Finnish-developed, open-source coronavirus vaccine nearly ready for testing, yle.fi 2020508 “The team of professors developing the vaccine are foregoing intellectual property rights to their work. In practice, they have gathered together research data in the field, refined it, added their own observations and are making it freely available.”
Finnish researchers introduce a nasal COVID vaccine, prnewswire.com 20210321
Cuba Vaccine Development
Cuba will begin administering its Soberana vaccine to 44K as a trial. Another Abdala vaccine will begin trials later in March, and another two vaccines are in the works. Cuba starts final-stage trials of two homegrown Covid vaccines, ft.com 20210304
Vaccine Results Tracking in Israel
https://ourworldindata.org/vaccination-israel-impact

Discrepancy in Article from New York Magazine
Vaccine prevents 98.9% of COVID-19 deaths — Israel, dw.com 20210220. Yet, with 50% of the country fully vaccinated, they sure are getting a lot of new cases every day.
The third wave of deaths in Israel was caused by the British B.1.1.7 variant. “The country locked down again in December after the spread of the more contagious British variant of the virus prompted a third wave that was the worst of all.” Israel’s First Covid-19 Vaccinations Were Easy. Now Comes the Hard Part. wsj.com 20210316

Asymptomatic vs Symptomatic Immune Response?
Feb 07, 2021
Why The Sudden Influx of New Variants?
March to August, mutations to the spike protein were not recorded, and now suddenly we have a whole new collection? That's very peculiar. There was only one more contagious single nucleotide COVID-19 mutation that existed before march 2020 and went on to become the predominant world strain by July.
Related articles:
Why some labs work on making viruses deadlier — and why they should stop, 20200501
Did the coronavirus leak from a lab? These scientists say we shouldn’t rule it out. MIT Technology Review 20210318
COVID-19: A wake-up call for biosafety, gmwatch.org 20200413
Who Are the Covid Investigators? Members of a WHO origin probe have conflicts of interest. wsj.com 20210215
List of Variants on Wikipedia
One need only take a look at history to see what people will do for greed. We take war for granted, but if you really think about it, it's organizations going out to kill people for resources. Killing innocent people is an acceptable risk in wartime. Morality goes out the window. How can someone excuse that? But they do. It's not far fetched with the pharma industry profiting from the virus, that they may be acting badly. Maybe the virus mutated by itself, maybe the mutation was released accidentally, maybe on purpose. People ignore reality and put their head in the sand to feel safe. They also want to believe in a higher power that will take care of them, so they feel incredibly happy to get the mostly untested vaccine.
New variants currently spreading are supposed to be the result of evolutionary pressure. The recent mutations in the virus has increased its contagiousness, being able to better attach itself to cell walls. Wouldn't a mutation of this kind have been favorable, if it had originated early on in the pandemic? Why such a long period of time without a spike protein mutation, and now, three almost simultaneous mutations being found in UK, South Africa, and Brazil? This sounds incredibly strategic for the vaccine manufacturers, who were going to market with a vaccine for a virus which the population had nearly achieved herd immunity.
The new mutations are also able to partially evade existing immunity, which will mean more business in future orders for the updated vaccines, while presently, pharma publishes studies about how their vaccines are effective for all variants.
In the UK and in South Africa, these new variants appeared when there was few daily cases occurring in the population, reducing the statistical chance for a more virulent mutation. Google the worldometer charts and see the timeline. It's not an impossibility that the mutation occurred when it did, but it's like the virus won the lottery by buying the one remaining lottery ticket.
Is the spike protein mutation on a multi-purpose gene?
Are Variants Responsible for the Increased Pandemic Intensity?
In the “progression of the pandemic by region” figure near the top of this page, we see in Europe an increase in pandemic intensity starting in late September and culminating in November. Was this explosion caused by the new variant B.1.1.7?
Did B.1.1.7 also cause the increase in NYC? The data least likely to be tampered with, and the data that best represents the pandemic, as noted in previously dated entries, are the hospitalization and deaths data. Especially for individual cities that were most affected. If herd immunity was achieved by these cities, they would not show a second wave as severe as the first, unless the virus presented as an entirely new antigen.

The chart suggests a partial immunity to the new covid variants. The second wave could be lower due to protective measures, but I don't think protective measures have as much of an impact as the public believe, especially with the increased contagiousness of new variants.
Alternatively, new variants may have little to do with the increase in deaths. New variants are not recorded as having spread much in USA (see CDC stats. In some countries the variants are quickly becoming predominant.
However, the data that proves the prevalence of new variants in USA is insufficient, due to very little case sequencing. NYC ”barely tests for virus variants” at 1% of cases (10% being the minimum recommended). In NYC, the UK variant B.1.1.7 was detected in 13 out of 1700 specimens. 1700 specimens is hardly anything when you have 5000 cases a day: what month period (170K / 5K = 34 days) were those specimens tested and what part of the city? USA may have a prevalent new variant of its very own, and it wouldn't be known due to lack of an organized effort.
Update 20210222:
Sweden latest wave of infections appear to have started late september, followed by an increase in daily deaths in late october (see worldometer). The B.1.1.7 variant made up 11% of sequences by the 4th week of 2021. The first case of 501.V2 (aka B.1.351) was sequenced January 3rd, and although the prevalence is increasing it is still currently a minority (5 of 581 sequences since first found).
“In Sweden, a variant share of 15.5% for week 5 was found as the average value across four of its southern regions (Skåne, Västra Götaland, Västmanland, and Gävleborg),[71] and under the assumption of 50% increased transmissibility compared to the original virus, the variant would become dominant around week 12–14.[94]” wikipedia.org
The B.1.1.7 variant would take around 10 weeks to increase from 10% to 50% of the infected population. Does this mean that 10 weeks before the 4th week of 2021, or the first week of November 2020, it had a 2% viral share? The timeline is off by a month for Sweden's COVID-19 increase in late September.
Maybe a previous variant was responsible for Sweden's increase? From the figure below, the D614G mutation doesn't seem to coincide with Sep-Oct. Unfortunately, I don't have enough evidence for causality.

Update 20210226:
“The head of the World Health Organization’s European branch says his organization expects a rising number of COVID-19 deaths in October and November.” WHO: European COVID-19 Mortality to Rise in October, November, voanews.com 20200914
This expectation was due to increased COVID-19 cases.
“France and its neighbours are grappling with a pickup in infections as people travel for vacations and attend summer gatherings. Officials are tightening measures to curb the spread but are reluctant to resort to the sweeping closures imposed during the initial peak of the pandemic in March and April.”Covid-19 cases climb in Europe as people travel for vacations and attend summer gatherings, straightstimes.com 20200823
Fortunately, the Oxford COVID-19 Government Response Tracker, created the Government Stringency Index and Containment Health Index. An example plot below.

I can guess that the authors of the index wanted to put a numerical value to real life transmission. So a 7 would be 20% less transmission than a 5, and a zero would be where people took no precautions whatsoever.
Maybe people behaving badly caused some of the increase in deaths seen for Europe in late September, but it wasn't until October that a new variant started taking hold. That brings the timeline closer to the start of November, where the B.1.1.7 variant is estimated to have gained a foothold.

Update 20210309:
There is mention, though no research study is cited, that the B.1.1.7 variant spreads 70% faster.
This is a quote by Elisabeth Mahase published on BMJ:
We’ve heard a lot about B.1.1.7 (first detected in the UK), B.1.351 (first detected in South Africa), and P.1 (detected in Manaus, Brazil), but other variants have also emerged, including one in New York. Named B.1.526, the variant contains the same E484K mutation that has caused so much concern in B.1.351. This mutation is thought to allow the virus to escape some of the body’s immune response. Vaccines developed against the original virus have also been found to be less effective against B.1.351 (table 1). In a preprint released on 25 February,20 researchers said the variant was “surging, alarmingly, in our patient population over the past few weeks” and that patients with this novel variant “were on average older and more frequently hospitalised.” They added that further analysis showed that the B.1.526 variant was “scattered in the northeast of US, and its unique set of spike mutations may also pose an antigenic challenge for current interventions.” Covid-19: Where are we on vaccines and variants? bmj.com 20210302
Update 20210325:
Sweden could have also achieved herd immunity, and had a second wave of COVID-19 due to the new variants, as they make up a majority of new cases:
“The variant B.1.1.7, first reported in the UK, was present in more than 50 percent of positive tests analysed in 13 regions, with the exact figure ranging from 16 to 72 percent between different regions. Variants first discovered in South Africa (B.I.351) and Brazil (P.1) had been discovered at a lower rate, only appearing in more than ten percent of cases or more in four regions.” New Covid-19 variants now dominate in half of Sweden’s regions, thelocal.se 20210316
Update 20210716:
Looks like I have to look through all the citations in this Wikipedia article to check for COI in the research. Even one researcher of many having ties to pharma would trounce the validity of the research. https://en.wikipedia.org/wiki/SARS-CoV-2_Beta_variant#Vaccine_efficacy
Update 20210801:
Although dated, a good review comparing older and newer variants of interest: What Scientists Know About the B.1.617 Coronavirus Variant, the-scientist.com 20210503
B.1.617’s double mutant moniker comes from changes it harbors that are similar to those in other known variants. One mutation, known as L452R, is also found in the B.1.427/B.1.429 variant first identified in California, where it has been associated with increased transmissibility. Another B.1.617 mutation, called E484Q, is similar to the E484K mutation found in the P.1 variant that was first detected in Brazil and the B.1.351 variant, also known as the South African variant. E484K is known as an “escape mutation” because it appears to help the virus partially evade immunity conferred by prior infection or vaccines, according to The BMJ.
Jan 22, 2021
Asymptomatics vs Unmasked Presymptomatic Super-Spreaders
“Many believe that asymptomatic transmission is driving much of the COVID-19 pandemic, which would suggest that viruses aren’t typically riding out on coughs or sneezes.”Face masks: what the data say, nature.com 20201006
There are issues with the previous quote. Who exactly is the “many”? The ratio of asymptomatic to symptomatic transmission hasn't had enough research to have any conclusion. Also, there is no mention that included in the term “symptomatic” are the presymptomatic, those which later develop symptoms. Overall, this nature article doesn't include anything that hasn't been heard already. Mask wearing mainly protects other people from getting a high dosage of a sick person's viral output. The following article correctly defines presymptomatics as symptomatics:
“For the purpose of epidemiological modeling, we cautiously suggest that at present, asymptomatics could be considered to have a degree of infectiousness which is about 0.40-0.70 that of symptomatics. However, it must be stressed that this suggestion comes from a very low evidence base and that estimates exist that are close to zero and close to 1.” The relative infectiousness of asymptomatic SARS-CoV-2 infected persons compared with symptomatic individuals: A rapid scoping review, McEvoy et al, August 2020
Do asymptomatic persons produce heavy viral delivery environments? Based on the theory that lower dosage transmission results in lesser disease severity, asymptomatic transmission among a population would lead to increased asymptomatic disease. Asymptomatic spread may work favorably towards herd immunity with a lesser death toll. However, most known transmission happens via superspreading events, where presymptomatic individuals with a high viral load transmit to the many.
Given that a UK door to door testing program found one in ten persons positive for COVID-19, asymptomatic spread could be an under-current that hasn't been measured, leading people to believe that COVID-19 only spreads via super-spreading events?
Percentage of Transmission Due to Super Spreaders With High Viral Load
Update 20210212:
“The amount of SARS-CoV-2 in a person’s body is a major factor in determining whether they are likely to transmit the virus to others, according to a study of nearly 300 infected people and their close contacts.” What makes a person with COVID more contagious? Hint: not a cough, nature.com 20210204 Which makes sense considering earlier research about most transmission occurring via super-spreaders.

Related:
Reinfections
Super Spreading Events and the Dispersion Factor K
Comment From Non-Stupid Person
Should the trial have been published? Some have turned to social media to ask why a trial that may diminish enthusiasm for masks and may be misinterpreted was published in a top medical journal. Woah! First, of all, I am prepared to die on the hill that science means publishing the results of truthful experiments no matter what they show. We can acknowledge limits, but we can never suppress results. Second, in today's environment of rampant conspiracy theories, watching doctors openly discuss not publishing results seems to be … I can't think of a polite word. Here's How to Think About the Danish Mask Study, medpagetoday.com 20201118
See this “living rapid review” article regarding the benefit of wearing masks:
Jan 13, 2021
Dominant New Variant in South Africa Could Evade Existing Immunity
A risk assesment from the Italians:
https://www.sanitainformazione.it/wp-content/uploads/2020/12/valutazione-del-rischio.pdf
The majority of the current wave in South Africa is from the new coronovirus variant 501.V2. This could suggest:
1. South Africa achieved herd immunity in the first wave (*)
2. The second wave is because the new variant presents as a new antigen, no longer affected by existing antibodies
3. The current vaccines won't work on the new variant
(*) note: South Africa's relatively low covid deaths per capita doesn't support this conclusion.
It's possible that in the UK, the latest wave of infections is also caused by new variant(s), but the beginning of the wave predates the discovery of the new variant in late september, although not by much. Maybe they didn't do enough sequencing to notice the new variant? For the non-scientists: testing for covid is not the same as sequencing the virus. In the following article they state that during August, when COVID cases were at an all time low, they had the capacity to sequence half of the COVID cases. However, I won't yet discard the possibility that the latest increases in daily cases in Uk, South Africa, and Brazil were caused by the new variants.
How do we collect and sequence SARS-CoV-2 samples? COVID-19 Genomics UK Consortium, 20201204
Update 20210125:
South African SARS-CoV-2 variant escapes antibody neutralization, news-medical.net 20210120 article based on the study:
SARS-CoV-2 501Y.V2 escapes neutralization by South African COVID-19 donor plasma, Wibmer et al 20210118
New SARS-CoV-2 Variant Could Evade Antibodies, the-scientist.com 20210122
And if they can evade the current vaccines, they can also reinfect those with immunity to the strain before the antigen mutations.
Note that the following study was made by employees of the Moderna vaccine. Due to the conflict of interest, the results are questionable.
mRNA-1273 vaccine induces neutralizing antibodies against spike mutants from global SARS-CoV-2 variants, Wu et al 20210125
Update 20210212:
“Antibodies from only five people could neutralize B.1.351. Following a single shot of the vaccine, however, participants’ levels of neutralizing antibodies against both forms of the virus increased by approximately 1,000-fold.” COVID research updates: Vaccines spur antibody surge against a COVID variant, nature.com 20210212
This is actually bad news. Although ten persons is not a sufficient sample size, the consequence would be that half the immune population produce antibodies that are not effective to the new variant. Not only will their immune response be ineffective, but it will also weaken their immune response. Producing non-functional antibodies is very taxing. See original antigenic sin.
Update 20210217:
I have not been pushing a fringe hypothesis for at least a month, as I found an article by Nature that gives the same conclusion: Fast-spreading COVID variant can elude immune responses, nature.com 20210121 “Pseudoviruses with the full package of 501Y.V2 mutations were fully resistant to convalescent serum from 21 out of 44 participants, and were partly resistant to the vast majority of people’s sera, Moore’s team found. There is now proof of several reinfections with 501Y.V2 in South Africa, says de Oliveira. It seems increasingly likely that the variant’s ability to spread in places hit hard by earlier waves of COVID-19 is being driven, in part, by its capacity to evade immune responses that developed in response to earlier versions of the virus.”
Although not yet studied, COVID-19 specialized T-cells may partially make up for the ineffective antibodies in some individuals reinfected with the new variants.
Dec 18, 2020
Testing in UK Could Now Represent the Pandemic
Case numbers, having been a favorite among the news media, could actually become a metric of some significance. Testing capacity has increased in the UK to the point where case numbers may be extrapolated to be representative of the pandemic. I was told they where testing 400K weekly in England, going door to door. *If* they are going door to door, then the case numbers can be extrapolated because the sampling is more representative of the population. I am not sure what percentage of the testing is done door to door, or if testing is compulsory.
Bradford door-to-door tests 'help to hit Covid targets', bbc.com 20201127
U.K. Sends Contact Tracers Door-to-Door to Track Spread of Virus, bloomberg.com 20200810
Door to door Covid testing starts in Birmingham hotspots, birminghammail.co.uk 20200913
Door-to-door 'coronavirus tester' hoax circles the globe, boosted by local media and police departments, nbcnews.com 20200323
England has a population of 56 million, so 400K per week is about 0.7% of the population. Comparing testing capacity per capita, by country, UK is at the top:

Update 20210106:
Note that for the UK, the positivity rate has been increasing since early September:

source
New Variant Found
New variant was first spotted in late September:
https://www.bmj.com/content/371/bmj.m4857
How common is it?
“As of 13 December, 1108 cases with this variant had been identified in the UK in nearly 60 different local authorities, although the true number will be much higher. These cases were predominantly in the south east of England, but there have been recent reports from further afield, including Wales and Scotland.
Nick Loman, professor of microbial genomics and bioinformation at the University of Birmingham, told a briefing by the Science Media Centre on 15 December that the variant was first spotted in late September and now accounts for 20% of viruses sequenced in Norfolk, 10% in Essex, and 3% in Suffolk.”
How accurately could they be tracking viral mutations? “On average, between 5 - 10% of all SARS-CoV-2 viruses have routinely been sequenced in the United Kingdom and 4% routinely sequenced in South East England since the beginning of the pandemic.” SARS-CoV-2 Variant – United Kingdom of Great Britain and Northern Ireland, 20201221 Although, if they have been going by case numbers, the percentage for sequencing rate is lower.
Update 202102:
Is there an increase in false negatives for variants that do not test well, reducing the number of samples to be sequenced of certain variants? The possibility appears to be minor: FDA: Coronavirus Variants May Cause False-Negative Tests, medpagetoday.com 20210108
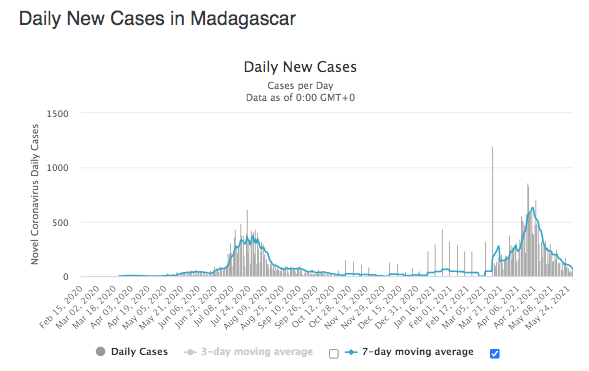
The date the variant spread into existence could also be off. Looking at the UK daily new cases chart from worldometer, could the new variants account for the latest wave?
https://www.worldometers.info/coronavirus/country/uk
I explore these possibilities because I am not satisfied with mainstream explanations for the latest wave of infections. I think there has to be something more to it, than a direct correlation of viral spread with easement of social lockdown. Given a variety of cultures and values, I don't think people are capable of following lockdown orders that strictly, so I think the months of diminished covid-19 spread after the first wave had as much to do with herd immunity as with lockdown. I could be completely wrong, but I will follow my hunch and document what I find as evidence, that the new wave of infections has to do with a new variant, which is either more infectious and/or presents at least partially as a new antigen.
Update 20210106:
Currently, experts are also looking at another variant of the virus that’s present in South Africa (https://www.cbsnews.com/news/covid-vaccine-new-strain-south-africa), 501.V2. This mutation (also located in the spike protein) may be more significant than the UK’s B.1.1.7 and therefore is the most worrying to experts. “This strain has fewer mutations than B.1.1.7 — three compared to 17,” says Nate Favini, MD, the medical lead of Forward (https://goforward.com/), a preventive primary care practice. “Scientists believe that the vaccine will probably still be protective against B.1.1.7, but are less certain about 501.V2 because there are meaningful changes to the shape of the spike protein in this variant. Source: What You Need To Know About The New COVID-19 "Super Strain", refinery29.com 20200105
Related article: List of Variants on Wikipedia
New Article About Human Stupidity
While I do not share the author's value system, I celebrate his clarity and objective approach to human stupidity, which could be said to be the main focus of this article as well.
https://claireberlinski.substack.com/p/the-coronavirus-europe-and-the-united
Reinfections
It seem that for influenza, everyone knows that for the same virus, you only get infected once. There are viruses where only children get sick, because older people became immune to the same strain of virus in their youth. But politics and fear is too strong for coming to logical conclusions when it comes to COVID-19.
It's not the first time I'm covering this topic, but this following article caught my attention, because it talks about persistent antibodies, memory b cells, and persistent t-cells. Something other articles about reinfections completely fail to mention. To its credit, the article is an excellent review of the pathways to reinfection, even if they are just academic without practical application.
“He says being reinfected might even be a good thing, “since you will continue to boost and train your immune system.””
Maybe people should continue living like normal, without lockdowns, so people can maintain their immunity?
What this article lacks, is any proof that reinfections make up a significant percentage of the pandemic. It could be a lot of talk about negligible risk. On the other hand, it could be the reason for the second wave of infections (along with new viral variants/strains).
However, for all the talk, even in Qatar, which according to this article has the most recorded per-capita cases of reinfection, only 1 in 500 people are affected (243 out of 142,308). Following the cited research, the abstract states: “Out of 133,266 laboratory-confirmed SARS-CoV-2 cases, 243 persons (0.18%) had at least one subsequent positive swab ≥45 days after the first-positive swab. Of these, 54 cases (22.2%) had strong or good evidence for reinfection. Median time between first and reinfection swab was 64.5 days (range: 45-129). Twenty-three of the 54 cases (42.6%) were diagnosed at a health facility suggesting presence of symptoms, while 31 (57.4%) were identified incidentally through random testing campaigns/surveys or contact tracing. Only one person was hospitalized at time of reinfection, but still with mild infection. No deaths were recorded.”
So in Qatar, only one person had an actual mild “reinfection”. I'm sorry, but I still don't believe reinfections have been a problem in this pandemic. Too much talk about singular cases, and no proof that there is an actual problem. People believe otherwise because of news media. Even the CDC states reinfections are rare. Though that may be changing in the future with new covid variants that evade existing immunity.
Due to the lack of individuals with reinfections, there are no studies about the possibility they may offer a vector for viral spread.
Ok, finally, I find an article that isn't based on disinformation: Sterilizing Immunity and COVID-19 Vaccines, verywellhealth.com 20201224. I don't supply a quote here, because the entire article is worthwhile reading. I only part way with the article, by adding the following statement: While the ability to be contagious upon reinfection is a possibility, the research suggests that the risk is negligible compared to first-time infected persons.
I read that reinfections are very difficult to prove, however, the UK has been sequencing between 5% to 50% of its covid cases (depending on the number of cases per week, which dwindled to very few in August). Surely these cases have identification attached? Bureaucracy truly is that inept? Something doesn't add up here. If there are or are not reinfections, they are not being tracked. If they were tracked, I think they would show that persons having previously recovered from COVID-19 have partial immunity to new covid variants, and are either asymptomatic or endure mild symptoms before recovering.
Update 20210212:
Those who have recovered from COVID, or having had the vaccine, even on the off chance of getting reinfected and having a miniscule viral load, could have a sort of covid-free passport, and not have to jump through regulatory hoops. However, the South African variant and its ability to reinfect half the existing immune population changes this possibility.
Update 20210301:
I found a study about reinfections in UK healthcare workers who had previously tested positive for COVID-19: Do antibody positive healthcare workers have lower SARS-CoV-2 infection rates than antibody negative healthcare workers? Hall et al, 20210115. These persons presumably would be exposed to COVID-19 more frequently than the rest of the population. They were tested every 2-4 weeks for nearly 5 months, between 18 June and 09 November 2020. The odds ratio of being PCR positive during this time period was 0.17. However, what isn't taken into account in the study, is that you can test positive for the virus, but not have any replication-competent virus. What was their level of contagiousness towards others? Did any others get sick from these participants? Surely they could have easily tracked and traced and provided results!
“The likelihood of recovering replication-competent virus also declines after onset of symptoms. For patients with mild to moderate COVID-19, replication-competent virus has not been recovered after 10 days following symptom onset (CDC, unpublished data, 2020; Wölfel et al., 2020; Arons et al., 2020; Bullard et al., 2020; Lu et al., 2020; personal communication with Young et al., 2020; Korea CDC, 2020).” (see The Contagiousness of Reinfected Persons may be on par with those Initiating Antibody Production in First Time Infections)
Related:
How Long Does Immunity Last?
Pre-Existing Immunity
COVID-19 Immunity Likely to be Long Lasting
News Media Crazy Talk
The possibility of transmission from reinfected persons has nothing to do with transmission by asymptomatic individuals, those infected for the first time. I state this having read some news articles that were just incorrect.
First time infected individuals, even if they remain subclinical throughout the infection, at first have not developed an adaptive immune response. Nor do they have antibodies specific to Sars-Cov-2. While they do not have antibodies, they can be infectious. But do they account for a substantial amount of viral spread? Maybe only those that go on to become symptomatic are the ones that spread the virus while asymptomatic.
“Conclusion: The infectivity of asymptomatic subclinical infection patients of coronavirus disease 2019 seems to be low.” Asymptomatic Subclinical Cases of Coronavirus Disease 2019 without Viral Transmission in Three Independent Families, dovepress.com 20200924 This study only follows three families, so it is not conclusive and I am still looking for more research.
The Contagiousness of Reinfected Persons may be on par with those Initiating Antibody Production in First Time Infections
I believe transmissibility of the virus from reinfected individuals may be in the same ballpark as those who are starting to initiate antibodies in their first infection. They are not contagious even while not yet having recovered from symptoms. The cough from these first-time infected, antibody producing individuals has been shown to not have a viral payload (I read this a while back and didn't record the source). It seems that in most cases, the immune system quickly gets the virus under enough control to significantly reduce chance of contagion: COVID-19 most contagious in first 5 days of illness, study finds, cidrap.umn.edu 20201120
https://www.obgproject.com/2020/03/26/how-long-does-it-take-for-covid-19-patients-to-develop-antibodies. Alternatively, another paper states: "IgM antibodies may take up to 10 days to develop and last 7–10 days." While this is for HSV, the immune system works the same, and is less vague than the obgproject.com paper. Please note IgM antibodies can convert to longer lasting IgG antibodies.
“The likelihood of recovering replication-competent virus also declines after onset of symptoms. For patients with mild to moderate COVID-19, replication-competent virus has not been recovered after 10 days following symptom onset (CDC, unpublished data, 2020; Wölfel et al., 2020; Arons et al., 2020; Bullard et al., 2020; Lu et al., 2020; personal communication with Young et al., 2020; Korea CDC, 2020).” Duration of Isolation and Precautions for Adults with COVID-19, cdc.gov 20201019
T Cells and Sterilizing Immunity
In influenza, sterilizing immunity depends on antigen specific T-cells. While immunity from one virus can give you partial immunity to a new related virus, you will likely have a mild infection before overcoming the new virus. Sterilizing immunity to influenza virus infection requires local antigen-specific T cell response in the lungs, Dutta et al, 20160906
I hypothesize the same would happen for Sars-CoV-2. In those immune to a certain Sars-CoV-2 variants, those re-exposed to Sars-CoV-2, even if having no circulating antibodies, would mount an adaptive immune response. Along with APC antigen presenting cells, CD4 T-cells initiate antibody production from specific Sars-CoV-2 memory B cells. Expanding roles for CD4+ T cells in immunity to viruses, Swain et al 01202012
”…we review studies indicating that CD4+ T cells control phagosomal infections asymptomatically in most individuals by secreting cytokines that activate the microbicidal activities of infected phagocytes but in a way that inhibits the pathogen but does not eliminate it. Indeed, we make the case that localized, controlled, persistent infection is necessary to maintain large numbers of CD4+ effector T cells in a state of activation needed to eradicate systemic and more pathogenic forms of the infection. Finally, we posit that current vaccines for phagosomal infections fail because they do not produce this “periodic reminder” form of CD4+ T cell-mediated immune control.“ CD4+ T Cells: Guardians of the Phagosome, Tubo and Jenkins 20140402
Related:
How Long Does Immunity Last?
Pre-Existing Immunity
COVID-19 Immunity Likely to be Long Lasting
Dec 11, 2020
Vaccine Benefits and Risks Are Mostly Untested
https://www.bmj.com/content/371/bmj.m4037
“None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.”
1) The vaccine trials are designed such that they are complete after reaching 150-160 “events”, or cases of covid, no matter how severe.
2) Severe cases make up a very small fraction of individuals who develop a covid infection, especially those whom the trials enroll: young healthy adults.
“Our trial will not demonstrate prevention of transmission,” Zaks said, “because in order to do that you have to swab people twice a week for very long periods, and that becomes operationally untenable.”
Does the vaccine create antibodies in the host? If it does, then I could make the same conclusion I've come to in previous posts, that once you have antibodies, the chances of being infected by Covid-19 are negligible.
However, there could be unwanted long term side effects. mRNA delivery in to host cells is highly experimental. Opportunities and Challenges in the Delivery of mRNA-Based Vaccines, mdpi.com 20200128
“When the world begins inoculating itself with these completely new and revolutionary vaccines, it will know virtually nothing about their long-term effects.” Could mRNA COVID-19 vaccines be dangerous in the long-term? jpost.com 20201117
What better way to advance DNA modification of human hosts than to use the public as guinea pigs? While mRNA doesn't change DNA, the advancement of the delivery systems is a stepping stone towards DNA modification therapies. The sky's the limit. I find the coincidence peculiar.


Update 20210202:
“During December 14–23, 2020, after administration of 1,893,360 first doses of Pfizer-BioNTech COVID-19 vaccine (1,177,527 doses in females, 648,327 doses in males, and 67,506 doses missing sex), reports of 4,393 (0.2%) adverse events after receipt of the vaccine had been submitted to VAERS.” Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine — United States, cdc.gov 20210115
Consider that going door to door, UK found one in ten persons positive for COVID-19. Consider that those who have had COVID in the past do not test positive as they have cleared out the virus. Consider a scenario where there is only one strain and variant of the virus: If at any one point in time there are one in ten persons testing positive, and time range for testing positive is a month, then maybe in 10 months everyone has already been infected? Granted, there would be a faster rate of infection with sufficient spread and with less of the population have immunity.
Let's ballpark that 70% of the UK was infected with Sars-Cov-2. Then the deaths make up 106,000 / 50 million = 0.2% death events. Comparable with the 0.2% adverse events for the vaccine, only with the slight detail that the adverse event is death. But hey, never mind that most people are already immune to the virus the vaccine protects against, there's money to be made!
In Israel, the vaccine would have more benefit because the local epidemic did not spread as thoroughly as in the UK. Israel currently has the most vaccinations per capita (55 per 100 persons), and while they have started delivering second doses, the immune system requires a few weeks to fortify from this second dose. Covid: Israel's vaccine rollout linked to infection fall, bbc.com 20210201 We'll have a better chart to look at in a few weeks.
We can only hope the vaccine does not have any long term health effects. I personally don't think there will be, but the mdpi article from Jan 2020 describes the dangers of the new technology.
Update 20210212:
Good news: “Out of the 523,000 fully vaccinated people, 544 were infected with COVID-19, of whom 15 needed hospitalization: Eight are in mild condition, three in moderate condition, and four in severe condition.” It works: 0 deaths, only 4 severe cases among 523,000 fully vaccinated Israelis, timesofisrael.com 20210211 Of course, the South African variant hasn't made headway in Israel, so that guarantees good marketing for pharma, for at least a couple months. Coronavirus: 80 cases of South African variant discovered in Israel, jpost.com 20210202
November 11, 2020
Erosion of Freedom
In the name of safety, human rights are being waived. I can predict this trend will continue, with technology and future crises as enablers. Surveillance technology especially. One can only hope that one faction is not significantly more powerful than another, and that some of the factions are supporting human rights.
People have different values. You're not going to get a Klingon to wear a mask. You have no right to expect them to be anything other than Klingon. The most you can hope for is that they take your need for mask-wearing into consideration, but that has to work both ways.
Since the coronavirus outbreak began, the condition of democracy and human rights has worsened in 80 countries, with particularly sharp deterioration in struggling democracies and highly repressive states, according to the experts surveyed by the project. More than 60 percent of the respondents predicted that the pandemic’s impact on political rights and civil liberties in their countries of focus would be mostly negative for the next three to five years. freedomhouse.org 20201002
While I think the media has been overblowing the severity of the pandemic, I have been underestimating it. However, in one of the worst affected countries, USA, the death rate from all causes has not been affected by a mean of more than ten percent because of COVID-19. These are not bad times. Much worse times will be had in the future with climate change. I wonder what life will be like in a decade or two, or for the newest generation among us. I wonder if climate technology would save us, much like human kind races to find a vaccine. Will the use of climate technology have unpredicted outcomes, and of what severity?

November 2, 2020
Is Something New Happening, part 2
Not specifically, but I am mainly considering if the virus has mutated to a new antigen, while being open to other interpretations.
As can be seen in the chart above showing deaths per day by world regions, something is happening in Europe. The rest of the world doing relatively fine while COVID-19 deaths in Europe going up? What? It can't just be Europeans behaving badly, right? Just Europeans not wearing masks and having sex parties?
Italy was one of the first affected in Europe, especially northern Italy in the Lombardy region with Milan. Hospitalizations in Italy are up overall:

But rather than thinking in terms of all of Italy, what would the above chart look like, if it was only for Lombardy? This I cannot find. Assuming herd immunity was reached in Milan / Lombardy, then while other regions of Italy may be progressing with the pandemic, Milan should be done with it.
Click for the much less significant positivity / testing rate data between March and present

The hospitalization rate would be best for gauging the severity of viral dispersion and disease intensity. The death rate should be decreased because medical care has improved in treating COVID-19.
In order to be 100% certain, that something new is happening, I would need some charts for European cities that have experienced the heaviest per capita hospitalizations earlier in the year, and are now having a second wave. I have had to go by per capita deaths in the past, because hospitalization data was not available anywhere during the earlier part of the year.
If the hospitalization rate has not increased significantly in certain cities or regions, while the rest their respective countries are having a new outbreak, then it could be concluded that these cities or regions have reached herd immunity. Rather than something new, the wave of hospitalizations for all of Italy would just be a continuation of the spread to regions that did not gain herd immunity.
I am rather disappointed, because I had hoped countries with the highest deaths per capita would not experience another wave. Italy is getting scary at 3 deaths per million per day, whereas, at the height of the pandemic, it was over 10 (note the logarithmic scale).

Italy's Lombardy region takes new virus measures, mainichi.jp 20201017 “Lombardy, Italy's most populous region, has once again become the most affected in the COVID-19 resurgence, adding more than 2,000 infections a day. Hospitals are coming under strain and intensive care units are filling up.” The news is grim, but I still want to see the severity by comparing Milan or Lombardy hospitalizations over time. Still searching for the data…
Update 20201113: Thanks to Liz Kalverda, I have found the data for London to compare to the rest of the UK. Unfortunately, the data is not per capita, so you can only compare the relative peaks. I would assume that London was the hardest hit earlier in the pandemic, having the highest population density in England, and being an international travel hub. So now I have New York City, London, and Sweden as regions where herd immunity was likely attained.
LONDON

source
NORTHEAST AND YORKSHIRE

source
Deaths from all causes data here
I could be mistaken, but I think the period of time where the pandemic was minimal, after easing off complete lockdown, was long enough in duration to show evidence of herd immunity. More than 5 weeks after easing off lockdown without an increase in hospitalizations would be sufficient proof?
The recent increases in disease could therefore be attributed to new Sars-CoV-2 variants with different characteristics in transmissivity R0, and dispersion factor K. Also, given that everyone's immunity to Sars-CoV-2 can be functionally different, perhaps a percentage of the immune population no longer has immunity to the new variant(s).
Liz said there is no evidence of mutation of the spike protein. But maybe it isn't just the spike protein. Maybe any change in the angle of the supporting structure of the spike protein would change the perceived antigen, for any antibody that nestles between two spikes.
Being a virologist, Liz Kalverda had the following thought: Sugars are involved in the viral attachment to cellular membranes. Even if the viral spike protein has not itself mutated, if the spacing between the spike proteins had changed, then perhaps this led to the virus having a more effective attachment to the cell membrane.
October 27, 2020
Is Something New Happening, part 1
Not specifically, but I am mainly considering if the virus has mutated to a new antigen, while being open to other interpretations.
I assumed the second wave below was a post-lockdown artifact, but now recently there is a third wave in daily deaths.


Though I thought it was unlikely, the virus may have formed into a new antigen? More awareness and testing has brought forth increasing death data, despite actual deaths continuing to decrease? Nobody knows. I would guess, without much certainty, that it is a continuation of the “case-demic”. Maybe the scare will last long enough to donate some money to those poor pharmaceutical companies.
Sweden has a ton of new cases, but not an increase in deaths:


For me to believe that there is something new happening, I would have to see evidence outside of USA's sphere of influence, and particularly, happening at cities that have already reached herd immunity, as covered previously in this wiki. Unfortunately, my source hasn't updated since Sep 25th.
covidtracking.com, 20201027 talks intelligently about rising cases, including hospitalizations. However, I still need an example of somewhere that has already been through the worst, and yet has rising positivity rates, hospitalizations, and deaths. So let's take a look at NYC:

In conclusion, “I'm shaking in my boots!” *smiley-face*. But before I laugh it off, let me consider that there is a boundless variety of antibodies and antigens. New variants/strains of the virus are emerging, and these new variants may have an antigen that doesn't quite match an immune person's antibody, thus creating a possibility for a second infection by SARS-CoV-2. Although not for everyone, because everyone can develop a different antibody.
While the possibility exists for a mutation to create an all-new antigen where the majority of the population will not be immune, it is not likely for coronaviruses. Coronaviruses are not Influenza. It’s Evolving: Coronavirus Genetic Mutation May Have Made COVID-19 More Contagious, scitechdaily.com, UT Austin, 20201101 There is one, and only one strain of SARS-CoV-2, virology.ws 20200507
September 10, 2020
MIT Covid-19 lecture Series
Bruce Walker
One thing that struck a chord with me, is when Bruce Walker says: “There are currently no highly effective treatments. There are some that have marginal impact, but we really need better drugs.” No mention of the MATH+ treatment developed by the FLCCC, which doesn't require any newly developed pharma drug, which would indeed carry a large price tag. The MATH+ treatment was applied to patients administered to ICU, and reduced mortality by 75%. If only the treatment was more well known, more lives could be saved?
Then he says that the reduction in the number of cases is because there is more adherence to mask wearing. Adherence to mask wearing? In the southern states? I seriously doubt that. Here in Brooklyn, less than 20% actually wear a mask correctly. Many southern states caught the pandemic later than northern states, but they are on the same trajectory: the covid death rates are declining from their respective peaks.
Then he talks about the duration of antibodies without mention of memory cells. He covers many topics saying there isn't enough evidence to come to a conclusion, yet he talks about COVID-19 effects on the lymph node germinal centers as if they are gospel. There are only some preliminary studies. No comparison is made with other viruses. If you investigate this further, leave me a note in comments section at the bottom of this article. I think this guy gets a lot of corporate funding.
You see him hesitating in his manner, when he talks about finding a population that has sufficient number of persons that can be infected, to test the vaccine. That’s because he knows what’s going down. Herd immunity is happening, de facto.
Veritas Medical Lectures
This is the video I watched: https://www.facebook.com/veritasmedical/videos/374536836892730
This guy with Veritas Medical is making quite a few interesting claims. I'll leave it to you to be the judge. I agree with some of his claims, especially the case-demic, which just highlights what I've also been writing about. However, his refutal of mask wearing doesn't take into account a lot of empirical evidence. I can't outright refute him without following all his research, time permitting
Veritas Medical Claim that the PCR Test is Ineffective
PCR detection of viruses is helpful so long as its accuracy can be understood: it offers the capacity to detect RNA in minute quantities, but whether that RNA represents infectious virus may not be clear.
During our Open Evidence Review of oral-fecal transmission of Covid-19, we noticed how few studies had attempted or reported culturing live SARS-CoV-2 virus from human samples.
This surprised us, as viral culture is regarded as a gold standard or reference test against which any diagnostic index test for viruses must be measured and calibrated, to understand the predictive properties of that test. In viral culture, viruses are injected in the laboratory cell lines to see if they cause cell damage and death, thus releasing a whole set of new viruses that can go on to infect other cells.
We, therefore, reviewed the evidence from studies reporting data on viral culture or isolation as well as reverse transcriptase-polymerase chain reaction (RT-PCR), to understand more about how the PCR results reflect infectivity. … Data are sparse on how the PCR results relate to viral culture results. Source: Are you infectious if you have a positive PCR test result for COVID-19?, Center for Evidence Based Medicine 20200805
Bits of virus can be found, but they may not be live. This is the case when the immune system has layed waste to the virus. These bits can have you test positive, even though you are not contagious. Virus garbage is eventually cleared.
So we’re looking at two different things:
The sensitivity and specificity of the PCR for detecting infection;
The sensitivity and specificity of the PCR for detecting infectivity.
This is just the start of our problems—because there’s a flip side. Some people may have a negative PCR and still be infected and even possibly infectious. If, for example, we check the wrong site (e.g. the nose and it’s now in the lungs) or there were tissue inhibitors of PCR present, or the sample was inadequate, then we may get a false negative. You may only think the gun is not loaded.
Welcome to the wonderful world of Clinical Medicine where, if you think it’s easy, you’re almost certainly doing something wrong. Dr Jo
August 12, 2020
Misguided Attempt to Convince Through Logic
I couldn't mention the words “herd immunity”, even a month ago, without outcry about how I just want to kill people. So this article has a lot to do with providing support for the idea that herd immunity is actually a factor in this pandemic. I provide support using the scientific method and logical reasoning. However, I think I am misguided in my attempts, when the receiver of the presentation does not function on logic. I'm just not good at creating a feel-good story that can sway the intuitive-visceral types, especially when the media has done such a good job at brainwashing them. That's a job for the marketing department.
How Long Does Immunity Last?
I am satisfied I've confirmed herd immunity does happen, and has already happened in many regions for COVID-19. But will it last? All the evidence points to long term immunity, but this conclusion is not 100% certain. In monkeys, the immunity lasts and will not lead a population to have a second wave of infections. Lack of Reinfection in Rhesus Macaques Infected with SARS-CoV-2, Bao et al 20200501
Concerns about Waning COVID-19 Immunity Are Likely Overblown, Scientific American 20200731
Can I Become Immune to COVID-19, popsugar.com 20200820
Vaccinations
The irony, is that by the time the vaccine arrives in 2021, most regions will already have herd immunity. Still, there are regions that have successfully contained the virus through mask wearing and contact tracing. Vaccines normally take 10 years to develop, so it is impressive that the world has fast-tracked vaccine development into just one year.
Regions that have held out with minimal spread of COVID-19, could now take the Russian vaccine. However, the Russian vaccine was only tested on 76 humans. Phase 3 clinical trials in USA require testing about 3000 people, to verify safety. Sometimes, an adverse effect only occurs in a fraction of subjects. Even if an adverse effect occurs in 1 out of every 5000 persons, and 60% of the human population got the vaccine, it would affect 1 million people… although they would stop vaccinating people before that happened?
Russia offers to help US with Covid-19 vaccine; US says no, cnn.com 20200813
August 11, 2020
Searching for Cities with a Second Wave
Updated September 25:

source
The slowing of infection rates in regions that have surged in the past suggests that herd immunity to COVID-19 is possible. The best example of herd immunity is Stockholm, Sweden. Preventative regulatory measures in Sweden have been minimal throughout the timeline. There has only been one wave of infections, and now barely a trickle of hospitalizations and deaths.
Another example is NYC, which is easing lockdown measures without a second wave of hospitalizations or deaths. However, NYC is taking intelligent action to re-open the city while reducing the vectors that research has shown to favor viral transmission. So perhaps a second wave has not formed because of the preventative measures. More likely, their big efforts would have made an impact had they pursued them *before* the pandemic.
I could estimate a theoretical upper limit of hospitalizations per capita, or upper limit of deaths per capita, as herd immunity is reached. Does a city's deaths rate and hospitalization rate decrease when approaching herd immunity?
In following the scientific method, I must look for evidence that disproves COVID-19 herd immunity is already occurring. Perhaps I can find a city that has had a large number of hospitalizations and/or a high death toll, and despite this, is now having another wave of infections.
My previous search involved comparing countries. However, the nature of this virus includes a low dispersion factor (K), such that it does not spread evenly across regions. Thus comparing cities, or densely populated regions, is likely more effective.
Among the cities with the highest death tolls per capita, I cannot find one that is currently having a surge in the fatality rate. There is no second wave anywhere. If there was one, it would have to at least be a third of the peak rate to be able to say anything. Cities just have one quick spike in infections.
Searching the news, hoping that the stupidity rate is also slowing, I am pleasantly surprised by a number of articles talking about herd immunity. For example, this this jewel of an article that says “Hark, herd immunity is slowing down the pandemic!”. From MIT no doubt, the people that deal with nuts and bolts and common sense.
Population immunity is slowing down the pandemic in parts of the US, MIT Technology Review 20200811
Related article: Good Covid-19 News From Italy...and Sweden, bloomberg.com 20200804
August 7, 2020
Correcting My Influenza IFR Error
There are always more infections than the cases accounted for. What I didn't know, is that influenza has a similar percentage of asymptomatic cases as that of COVID-19! I overlooked that the CDC figure for influenza is for symptomatic cases only, and thus a CFR rather than an IFR.
So instead of thinking COVID was about twice as deadly as the flu, I could see that it's much more deadly. I was estimating the COVID-19 IFR as 0.2%, and incorrectly comparing it to the flu CFR of 0.1%-0.18%. The IFR of the flu is about one quarter of its CFR. So while the number of people dead hasn't changed, if every pitch is a person getting infected, influenza simply has a worse batting average than COVID-19.
Click here for the calculation of influenza IFR
Given the number of deaths from COVID this year may be double that of a bad flu season, the IFR for COVID-19 could be as low as 0.1%. Also to be taken into account, is the difference in the percentage of a population required for herd immunity. This may be higher for COVID-19 than for influenza, not only because of a difference in transmissibility, or how contagious the disease is, but also because of a difference in the level of pre-existing immunity in the population. The belief that there is no pre-existing immunity to COVID-19 is incorrect. The new strains may not be more contagious, rather, a new antigen that evades existing herd immunity.
Pre-Existing Immunity
More evidence to topic previously covered in ”COVID-19 Immunity Likely to be Long Lasting“.
“Four independent groups of scientists—based in the U.S., Germany, the Netherlands, and Singapore—have now found that 20 to 50 percent of people who were never exposed to SARS-CoV-2 nonetheless have significant numbers of T-cells that can recognize it. These “cross-reactive” cells likely emerged when their owners were infected by other, related coronaviruses, including the four mild ones that cause a third of common colds, and the many that infect other animals.” Immunology Is Where Intuition Goes to Die, Ed Yong, The Atlantic 20200805
Superspreading Events and the Dispersion Factor K
Why do some COVID-19 patients infect many others, whereas most don’t spread the virus at all?, sciencemag.org 20200519
How ‘Superspreading’ Events Drive Most COVID-19 Spread, scientificamerican.com 20200623
Estimating the overdispersion in COVID-19 transmission using outbreak sizes outside China, Endo et al 20200710
If K is small, then most chains of infection die out by themselves and SARS-CoV-2 needs to be introduced undetected into a new country a number of times to have an even chance of establishing itself. “If the Chinese epidemic was a big fire that sent sparks flying around the world, most of the sparks simply fizzled out.” sciencemag.org
The dispersion factor could explain, in part, why some regions are spared, while others are COVID hotspots.
“As few as 10 percent of infected people may drive a whopping 80 percent of cases in specific types of situations … SARS-CoV-2’s transmission is not as reliant on superspreading as SARS and MERS were but is far more dependent on it than influenza … Researchers have identified several factors that make it easier for superspreading to happen. Some of them are environmental. For instance, poorly ventilated indoor areas seem especially conducive to the virus’s spread. A preliminary analysis of 110 COVID-19 cases in Japan found that the odds of transmitting the pathogen in a closed environment was more than 18 times greater than in an open-air space.” scientificamerican.com
While asymptomatic spreading makes containment more difficult, a smaller K and an understanding of superspreading events is critical in the success of track and trace efforts.
Policies to be Learned From the Experience of Others
- Protect the most vulnerable and the elderly
- Protect migrant workers living in cramped and shared housing
- Test, trace, and quarantine
- Wearing of masks in public indoor spaces
- Lockdowns have dire consequences including death from starvation among the poor
Iran Hiding True Number of Cases and Deaths
Coronavirus: Iran cover-up of deaths revealed by data leak, bbc.com 20200803

Their death rate is about three times what they are reporting. So Iran actually has 683 deaths per million, which would put them neck and neck with the UK. However, Iran is just cresting its second peak in daily deaths, so they now look like the top contender for the gold medal.
Contracting COVID-19 While Mask Wearing May Reduce Chance of Death
Populations that have adopted mask wearing, not only do they have less cases, but they also suffer a lesser percentage of cases that end in death.
Covid-19: More cases than UK, Spain, Italy - but South Africa has lower mortality rate - we asked experts why, health24.com 20200723
Face masks could be giving people Covid-19 immunity, researchers suggest, telegraph.co.uk 20200912
Global COVID-19 Case Fatality Rates
This section dedicated to this article: Global Covid-19 Case Fatality Rates, cebm.net 20200609, which has a chart displaying the CFR's by country, including Singapore and Katar, which have only had young populations affected, and thus have very low case fatality rates.


Considering those over the age of 65 are 10 times more likely to die of COVID, Qatar and Singapore are not that out of line. These two countries also have the most thorough testing of any nations, according to the “events per 100 observations” column. However, despite having the most thorough track and trace, I think that for every case they find, they could be missing 2 cases.
Notice my estimate for an IFR of 0.2% is within the bounds of this chart.
Case of the Missing Cases
Reasons for virus or antibody testing efforts to miss cases:
- Lack of sufficient testing
- Only the symptomatic are tested
- T-Cell immunity
- Antibody immunity with diminished blood counts
Even with adequate track and trace testing, cases can still go unnoticed:
- All event attendees are not always known
- Non-superspreading events are still possible by chance public encounters and by undisclosed encounters
My prediction is that herd immunity is being reached, where the pandemic is further widespread than estimated, and herd immunity requires less of the population than estimated. The section on herd immunity threshold covers the phenomena of non-homogenous mediums, and the reduced requirement of natural immunity as opposed to vaccinated immuniy.
August 5, 2020
Will Spain Have a Second Wave of COVID-19?
Just when I thought everything was right in the world, that herd immunity had been reached in countries with the highest deaths per capita, Spain has to go and ruin everything. Esos Españoles son tramposos!
Spain cases and deaths: https://www.worldometers.info/coronavirus/country/spain
Spain positivity rate: https://ourworldindata.org/grapher/positive-rate-daily-smoothed?tab=chart&country=~ESP
Spain regions of infection:
https://cnecovid.isciii.es/covid19
https://www.nytimes.com/interactive/2020/world/europe/spain-coronavirus-cases.html
As for hospitalizations, I can't find anything but a news source showing a doubling in the COVID-19 hospital admissions rate, between July 12-22: Coronavirus crisis in Spain: data from 10 regions shows rise in cases and hospital admissions, elpais.com 20200724
” It is important not to compare the absolute figures from March and April, given that detection is much better today and a greater percentage of cases are being identified. “In March, for every case confirmed by PCR tests there could have been 10 (if not more) who were not diagnosed. Now we are sure that the number is much lower,” explains Rossell. “
It's too bad you don't have the data on hospitalizations, señor Rossell. It would be useful to compare the present to the heights reached in March and April. I guess we will just have to use the deaths data as it starts to trickle in.
Is this new wave happening in provinces that were not affected previously? New York Times itemizes the deaths and case counts per individual provinces in the following tables:


The case counts cannot be compared between March/April and the present, so I will once again assume that regions with the highest deaths per capita are near herd immunity.
The action is happening in Aragón, which has had half as many deaths per capita as the worst affected provinces. I can estimate that Aragón needs to approach herd immunity by obtaining a death toll closer to the provinces of Madrid and Castille-La-Mancha. However, the population of Aragón is small compared to other provinces. So based on Aragón, I could predict that the coming wave of daily deaths will be small compared to the height of the epidemic in Spain.
I hope there aren't other provinces that need to turn in a late death toll homework assignment. If the same were to happen in Andalucía, the most populous province of Spain, and also one of the lowest in deaths-per-capita, the situation would elevate Spain to levels greater than any other country.
That would put a big hole in my hypothesis, that herd immunity was close to being reached by countries with the highest deaths per capita. It well may be that a larger tide of cases and deaths is being held back by a new normal of mask wearing and contact tracing. While I have been comparing countries, more accuracy could be had by comparing cities. The results may be rather scary.
But let me not be so fatalistic. Maybe the lack of congruity in the data from different regions of Spain, has more to do with the lack of reporting. Maybe the virus has already spread to all of Spain? Take a look at this article: More Than 90% of People Who Have Tested Positive for COVID-19 in Andalucía Showed No Symptoms, theolivepress.es 20200702 So there, I was being fatalistic for nothing.
Contagions in Spain Multiply by Eight 40 Days After the Tip of the State of Alarm, pledgetimes.com 20200811
This article tells you as a matter of fact, that the increased number of cases is due largely to increased testing, that the number of hospitalizations are nowhere near the peaks reached beforehand, that some small increases are to be expected from the end of the lockdown.
In contrast, articles like this one are scary sensationalism: The number of infections, deaths, hospitalizations and patients in intensive care continues to rise, with the cumulative rate of Covid-19 now nine times higher than what it was in mid-June, elpais.com 20200805
Update 20200823: As expected, no second wave of daily deaths is occurring in Spain. The death rate has increased very slightly, but nowhere near the level of the first wave (not even 1/25th the highest death rate), suggesting that the large increase in cases is an artifact of increased testing. If I looked up hospitalizations, I would see the same.
Another Look at COVID-19 Deaths vs Population Density
The population density of Andalucía is very low compared to Madrid, but that of Castille-La-Mancha is even lower. Castille-La-Mancha's largest city has only 150K inhabitants and a density of 150/km^2, which pales to the size of the size and density of the largest city in Andalucia. Yet despite its very low density, Castille-La-Mancha managed to have the highest deaths per capita in all of Spain. Once again, population density and transmission are not showing a correlation, so there must be larger confounding variables.
August 4, 2020
Considering a Social Aspect to an Increasing Positivity Rate
As covered previously, testing has expanded across USA. There may be no limit to the number of tests that can be conducted on those who present themselves for testing. The matter may be getting people to go and have themselves tested.
In the beginning, with the mass hysteria and panic brought on by the news channels, people went to get tested because they thought they were likely going to die from getting sick with COVID-19. Case Fatality Rates as high as 20% were publicized by the media. “I have a tickle in my throat, OMG, I need to go to the hospital!” In early April in NYC, those frightened individuals were turned away, and told that if they don't have a fever, they don't have COVID-19. That was when there was a testing capacity shortage.
Question at Quora, late April: ”If the US medical community is sending people with non-severe symptoms of COVID-19 home without testing, then are the numbers of COVID-19 positive much higher than what’s being currently reported?
Despite the expansion in testing, many states still do not test a sufficient number of cases. The percentage of tests that are positive should remain constantly low, if they are testing a sufficient amount of the population. WHO recommends 5%, assuming surveillance for suspected cases is comprehensive. This means that ideally, the amount of testing would increase or decrease with the amount of existing COVID cases in the population, which would mean tracking an unknown number of cases with time. At least in theory.
If the following chart from Our World In Data is accurate (which is in question), then the steep drop in the testing positivity rate should indicate that testing capacity became nearly sufficient around mid-May. The chart represents the USA average. Individual states have fluctuation in the positivity rate depending on the state and the calendar day, which can be seen at John Hopkins: Which U.S. States Meet WHO Recommended Testing Criteria?.

Mid-May to mid-June was the golden era, where people were sufficiently frightened to go get tested even if they were feeling just-a-bit-off.
Now, the word has spread that the chance of ending up dying or in ICU, is much much lower. People are still panicked, but are willing to wait and see if they are actually sick. Which represents a problem. How are you going to keep the positivity rate low, at the WHO recommended level, if only the bloody sick are showing up to be tested?
An example of this hardship, is the empty testing capacity in Arizona: “Federal, state, and local government agencies continue to provide free diagnostic testing in Maryvale and South Phoenix – the two testing sites launched on Friday. With both sites operating throughout the weekend, there have been minimal wait times and plenty of available appointments. Up to 5,000 tests can be conducted each day – 2,500 at each site – to serve up to 60,000 Arizonans. As of Tuesday morning, only 5,537 of the 20,000 available tests since Friday have been used.” az.gov 20200721
It's really curious that they can't get people in Arizona to use up all the available free tests. It seems they are exhausting the population that have the inclination to get tested. They are offering free tests, but people aren't showing up.
The increase in the positivity rate may not have to do with increased prevalence of the disease, but more to do with social opinion of hospitals and government. People can't stand to deal with bureaucracy so much, that they would rather die of COVID-19.
Another reason people may not want to get tested, is that COVID-19 has a negative stigma associated with it. With all the news of reinfections, people who continue to get sick from COVID, it is easy for many to have the impression that COVID is like a venereal disease that's going to follow you for the rest of your life.
Maybe they want to stay as far away as possible, from people that are going to get tested for COVID-19. Maybe they would rather not know, where knowing means having to isolate yourself for weeks.
So you end up with patients coming in via ambulance, because they procrastinated getting tested as long as they could. This in turn, gives you a higher positivity rate, and testing clinics sitting around twiddling their thumbs.
“Why have numbers plummeted so drastically? “We don’t really know why,” says Ryan Kiessling, BRF’s operations manager. “It seems to be fatigue.” That’s probably a pretty good theory. According to a Gallup poll this month, many Americans think the situation in the US is getting better. With more businesses and more recreation areas like beaches opening up again, people are more willing to let their guard down and abandon the wearying habits they’ve kept up for several months: they are increasingly resuming regular activities, and the number of Americans practicing isolation dropped from 75% to 58% in May. And that also means they may view testing with diminished importance. “People are just feeling really tired about anything that has to do with covid at this point,” he says. “They just want it to be over, even though it’s not.” ” The US now has more covid-19 tests than it knows what to do with, technologyreview.com 20200627
Send Children to School, or Keep the Pubs Open?
In UK, the government is considering keeping kids from going to school, because otherwise they can't also keep the pubs open. It's a matter of national priority. Coronavirus: Pubs in England likely be exempt from any new restrictions, independent.co.uk 20200804 Alcoholics Anonymous is also banned from having home meetings. Let's give a toast to the UK!



The Death Toll to Achieve Herd Immunity in the Big Apple
NYC went viral this spring. Viruses voted NYC as one of the top vacation spots. The density of unmasked juicy New Yorkers was to die for. Subways packed like sardine cans, small indoor spaces, loads of restaurants and entertainment venues. It was a truly remarkable season.
Click here for Intro to Herd Immunity Threshold 101

The deaths peak is over 600% above the normal rate for all causes of death. Now there's a pandemic to write home about!!

August 1, 2020
News Articles About Herd Immunity? Preposterous!
The writing has been on the wall for long enough. The solipsistic, being super creative, may be able to persist with cognitive dissonance indefinitely. However, if the scientific method has its due, many of those having come to dubious conclusions driven by fear and self-preservation, will be pressured to invoke imaginative thinking, the likes of which will exclude any personal accountability.
News sources have a financial conflict of interest in cultivating cliffhanger drama for readers to come to day after day. The New York Times, having milked this drama out for as long as possible, is starting to allow some sanity to surface. I find it interesting that an article covering textbook science by two professors of immunology at Yale University, is published in its “opinion” page.
Scared That Covid-19 Immunity Won’t Last? Don’t Be, nytimes.com 20200732
“Dr. Mina had choice words for the physicians who caused the panic over reports of reinfections. “This is so bad, people have lost their minds,” he said. “It’s just sensationalist click bait.”” Can You Get Covid-19 Again? It’s Very Unlikely, Experts Say, nytimes.com 20200722
I don't think herd immunity is something to work towards. It is happening on its own. It can be slowed down with draconian measures, but at too great a cost. Forced lockdowns are more detrimental to the poor than the virus is on all others combined. Compulsory mask wearing takes away freedom. I believe the worse outcome is taking away an opportunity for growth. Progress towards a better society can only take place where individuals have the responsibility to protect each other. Including protecting each other from the pervasive conflict of interest imposed by instinctual behavior and capitalism.
Chinese Article on Sweden
The start of school under the new crown epidemic: inspiration from Sweden, ifeng.com 20200720
Click here for english translation, if above link disappears
July 28, 2020
Hospitalizations !!!
Wow, why did I not see this in the news before? They have data on the number of hospitalizations for USA COVID patients? That could be better than the deaths data, because, among other variables, doctors are learning to better treat the disease.
Apparently, the hospitalizations data comes from a CDC project called COVID-NET: COVID-19-Associated Hospitalization Surveillance Network and has a disclaimer that includes only covering approximately 10% of the US population.
Click here for full disclaimer

Now, see how nicely that compares with the daily death data? A big hump, followed by a second smaller hump. As expected, the second hump is proportionately smaller in the daily deaths chart. Feel free to replace the word “hump” with “wave”.

Then comes Covidtracking.com from Atlantic Magazine. They are supposedly doing what the CDC could not: tracking all the data. See their message. The hospitalizations chart is different than that from the CDC, perhaps because they are following hospitals in hot spots that the CDC isn't. You can't be too hard on the CDC: Cuts to Prevention and Public Health Fund Puts CDC Programs at Risk,the-scientist.com 20180209
Liz Kalverda, virologist, brought up a good point. If you test positive for COVID-19, does that automatically get you hospitalized? During the beginning of the pandemic, it was a UK policy to hospitalize everyone with COVID, which is probably why they managed to kill so many people. This is likely not the case in USA.
Trump F%%ks Up the Data
When you are collecting data, you need some semblance of consistency. I don't care how messed up each state's methods are, so long as they continue to be messed up in the same way. Trump has ordered hospitals to send data directly to a company named Teletracking. I can imagine that their funding depends on being agreeable to the Trump administration. Going forward, I don't know if I will trust any data. The Time Magazine article has given its best effort in unbiased reporting of the situation.
New York Times article Where the Virus Is Sending People to Hospitals states: “Public health experts say detailed local data on where people are hospitalized — a real-time measure that does not depend on levels of testing — is crucial to understanding the epidemic, but federal officials have not made this data public.” Can I assume this is because the CDC no longer has access to the data?
Who's Currently Taking a Beating?
Click to sort by columns, and there is a slider at the bottom where you can adjust the dates:
7 Day Rolling Average of Confirmed Deaths Per Million by Country, ourworldindata.org
Another site, providing John Hopkins data:
New Deaths from COVID-19 per Day, normalized by population, 91-divoc.com
Is Worldometer a Reliable Source?
In regards to John Hopkins University's use of Worldometer data: “I think JHU has been under a lot of pressure to update their numbers,” he said. “Because of this pressure they have been forced to or incentivized to get data from places that they shouldn’t have, but in general I would expect JHU to be a fairly reliable source.” Quote from Edouard Mathieu, the data manager for Our World in Data (OWID).
A Short Review of COVID-19 Data Sources, towardsdatascience.com 20200327
July 17, 2020
Face masks are not needed outdoors
Do I Really Need To Wear A Mask Outdoors? Here’s The Science, forbes.com 20200630
We Need to Talk About Ventilation, theatlantic.com 20200730
Schools Beat Earlier Plagues With Outdoor Classes, nytimes.com 20200717
Uruguay and Cuba Are World Leaders in Health Care
Sars-COV-2 is Not a Proviris
Due to the mass-hysteria in the public, misinformation has been spreading that once you have Sars-COV-2 you have it for life.
HIV and chickenpox are proviruses. They integrate into the host DNA. Coronaviruses are not proviruses. Once you are over COVID, you do not have a life-long affliction.
COVID-19 2021 Safety Patch, to be worn at all times:

Liberals don't seem to like this series of posts, even though I'm providing evidence to improve the situation. Perhaps they are convinced I'm trying to trick them? Many liberals have become what they supposedly abhor: close-minded. There's a genetic trait that predisposes someone to be uncomfortable with ambiguity. They are typically conservative, but if you grow up in a liberal environment, you are actually a conservative in liberal clothing.

July 12, 2020
Death Lags Cases, But Only if the Testing Rate is Constant
The article from The Atlantic: COVID-19 Cases Are Rising, So Why Are Deaths Flatlining? has the hypothesis that the reason the number of daily deaths has not increased with time, is that deaths lags cases. This is true, as in the case of Iran covered in a previous entry, the lag was between 4 and 6 weeks. However, Iran was the only country I could find as an example of this. Many other countries had an increased rate of cases, but no increased rate of deaths.
The Atlantic article places too much importance on the lag time, saying “that might explain almost everything”. I think it is more likely, that the increased amount of testing is revealing more cases.
The limited amount of testing in the past did not fully capture the pandemic. The testing capacity was only sufficient for the critically ill. Many less severe cases went undiagnosed, and recovered without treatment. With increased testing, more of these hidden cases were counted. The surge in cases only created the appearance that pandemic was growing, when it had been of great magnitude all along. I've covered other reasons for increasing number of cases relative to deaths, but I believe this one point is overly underestimated.
There may have also been deaths that were not counted as COVID-19 related, because the disease was thought to be only a respiratory infection. However, I think the number of cases of deaths was dwarfed by the number of asymptomatic and untreated cases that went untested early in the pandemic. Countries experiencing a second wave of cases, and no second wave of deaths, were only catching up to a real metric of COVID cases occurring in the population.
In USA, The situation has changed dramatically. Currently, many states, such as New York, have opened up dedicated testing sites and are encouraging everyone to get tested, whether they have symptoms or not.
Click for Texas, Florida, and Arizona
USA Unlikely to Have a Large Second Wave of COVID-19 Deaths
New York Times has an ongoing map of the current regions worst affected by COVID-19. I'm fairly certain COVID has had time to establish itself in all metropolitan regions of the US for a few months, with the current hot zones being in the south.
Where the Virus Is Sending People to Hospitals, nytimes.com 20200723
Most importantly, the USA outbreak wave of deaths per capita was larger than that of Iran, comparable to countries that did not have a second wave of daily deaths coming out of lockdown. For this reason, I don't expect much of a second wave of USA deaths.
Increasing Percentage of Tests Positive for COVID-19
Update 20200722:
The New York Times opened my eyes to evidence that I overlooked. The percentage of tests positive for COVID should have decreased with additional testing. Instead, it has increased. Spike in U.S. Cases Far Outpaces Testing Expansion So an important pillar of support is knocked out for the improbability of a second wave of daily deaths.
What could be going on here? Looking at the testing data from John Hopkins, not all states are carrying out an equal number of tests per population size. The positivity rate could be affected if the testing was concentrated at the current hot spots, rather than spread homogeneously throughout USA. However, this does not appear to be the case.
This would mean that the actual number of COVID cases is increasing. People are returning to work, returning to restaurants and bars, participating in protests, or enjoying summer gatherings. Doing all the things that the Swedish have been doing all along, and then some.
An actual, real-life surge in the number of cases predicts that more deaths will follow. Maybe USA is bad at taking it easy, and the percentage required for herd immunity will be greater. Good evidence for herd immunity would be a decreasing positivity rate with a constant testing rate. Alternatively, a constant positivity rate with a diminishing testing rate.
Click for the other unlikely methods of estimating the level of immunity in a population
Click for a chart that confused me to no end

The Death Toll Required to Achieve Herd Immunity
Countries with high death rates early in the pandemic did not experience an increase in deaths after easing lockdown, and this could be attributed to herd immunity.
As mentioned previously, there are factors that favor a declining death rate. One is that doctors have more experience treating the disease. Another is that the most vulnerable were killed off early. Yet another variable, is that the number of deaths was underestimated earlier in the pandemic, so the initial wave in the rear view mirror appears smaller than its actual size.
A next step would be to compare the countries with the highest overall deaths per capita. Do they now have low daily death rates? If USA deaths per capita is getting close to the other big winners, then a second wave in daily deaths is less likely.
Belgium was overestimating deaths, and is thus disqualified. There's no way USA can beat UK, so I'd guess the US still has at most another 200 deaths per million to go. The second wave, if more than a speed bump, will not be as big as the first.

The Immunity Percentage Required Depends on Social Practices
Update 20200725:
I could be all wrong. Many believe we are nowhere near the level of actual COVID cases required for herd immunity. Maybe the reason that the countries with the most deaths per capita are now having low case and death rates, is that they are following the protocols required for containment, namely mask wearing and contact tracing. So lets take a closer look and see if this may be the case.
Mandatory Face Mask Rules Spread Across Europe Amid Uptick in Coronavirus Cases, time.com 20200724
Face masks: what are the rules in EU countries? cgtn.com 20200704
The World Is Masking Up, Some Are Opting Out, bloomberg.com 20200717
Click here for timeline of mask wearing rules in countries with highest death toll
The bloomberg article shows that Sweden is the only country with a continued lack of mask wearing and a cumulative high death toll. Denmark, Norway, and Finland got along without mask adoption by containing the virus with contact tracing after initiating lockdowns and closing borders. Thus only Sweden is a possible example of herd immunity, having few daily cases, where mask wearing is not a factor reducing virus transmissibility.
Did Sweden's coronavirus strategy succeed or fail? bbc.com 20200724
Sweden's herd immunity appears to have a lower percentage requirement than countries with larger per capita death tolls. Sweden has a reputation of being mostly rural, but this is not the case. The rural population of Sweden adds up to only 13% of the total.
Although never having a lockdown, the government chose select measures to reduce transmission optimizing safety and freedom of choice. Government workers that can work from home continue to be mandated to do so. Outside of government, however, public policy is based on recommendations.
One example, is DIY contact tracing. As of July 20th, Sweden chose to give individuals infected with COVID-19 the responsibility of telling others they have been in contact with. reuters.com 20200720
July 11, 2020
Accuracy of Using Death Data in Charting the Progression of the Pandemic
I had intuitively assumed the death data would be more accurate than number of cases, but I decided to investigate.
In the United States, “…public health experts say the method used to count deaths from a disease like Covid-19 is decades-old and some amount of uncertainty is simply part of the process. … Many more death certificates show Covid-19 as a cause of death but do not match up to positive coronavirus cases found through disease surveillance. If a person dies from Covid-19 without a lab test, that is a probable death. The C.D.C. has said probable deaths are a standard part of the counting process.” Is the Coronavirus Death Tally Inflated? Here’s Why Experts Say No, nytimes.com
Another article “How Are Covid-19 Deaths Counted” was published May 18-19, 2020, on both livescience.com and scientificamerican.com:
Both undercounts and overcounts of COVID-19 deaths are possible, Wolfson said, but it's not yet clear which is more likely, or whether they might simply balance each other out. Fowkes said that based on her experience, it's more likely that COVID-19 deaths are being missed than overcounted. That's because New York is among several cities that show spikes in deaths at home, and these anomalous spikes could be due to untested, untreated COVID-19.
Perhaps, the best clue as to whether COVID-19 deaths have been undercounted or overcounted is excess mortality data. Excess mortality is deaths above and beyond what would normally be expected in a given population in a given year. CDC data shows a spike of excess mortality in early 2020, adding up to tens of thousands of deaths.
Some argue that many of these excess deaths are related to COVID-19 lockdowns, not COVID-19 themselves, Faust said, because people fear catching the disease if they go to the hospital for other reasons. A study in the Journal of the American College of Cardiology did find that nine major hospitals saw a 38% drop in emergency visits for a particular kind of heart attack in March. That suggests that people really are delaying or avoiding medical care, which could mean that some of them die of preventable causes.
But non-COVID conditions probably don't explain most excess deaths, Faust said. Only a portion of heart attack visits would have represented lives saved, he said, because doctors must treat perhaps 10 patients to save one life. And other causes of death — such as motor vehicle accidents — are down.
This could change with time, Faust cautioned. For example, if cancer patients forego their treatments for a year, rather than a few months, the impact on their death rates is much more likely to be noticeable in the population-wide data. But for now, he said, “it's unlikely that the coronavirus deaths are being overcounted by a magnitude that explains our observation that something very unusual is going on.”
So the reason for the possible under-reporting of deaths is that “…many deaths occurred before we were able to test for the disease.” (Quote from Dr Fauci) What counts as a COVID-19 death?, wtsp.com. Which would mean, that with the current higher level of testing, this under-reporting should be much less or negligible.
Not to be confused with the over-reporting of CASES, covered on May 24th
Testing Rates Over Time
The amount of tests carried out, increases the number of cases found and reported, and affects the R0 models if they don't take into account the increased testing. The test subjects can range from only the very sick, to anyone that chooses to be tested, mostly depending on test kit availability.

July 5, 2020
Lockdowns Have Caused More Deaths Than COVID, Among the Poorest
“During the lockdown, India saw hundreds of deaths not due to Covid-19, but as a fallout of the measures taken” Why Covid-19 hasn't been the only killer during lockdown, indiatimes.com “Deprivation and distress caused by the total standstill, as captured starkly in the exodus of migrant workers back to their native places and the long lines for food and relief, were not without their share of tragic outcomes. Research by a group of volunteers shows India saw hundreds of deaths amid the crisis that were not due to Covid-19 directly but as a fallout of the lockdown itself.” The article talks about how the world's poorest are the hardest hit by loss of income.
I'd like to see the lockdown promoting, high-fear-homeostasis persons, promote that idea for the welfare of the poorest. Not going to happen. It will just be an uncomfortable fact brushed aside, while in their minds they continue in virtue. Even if lockdowns were necessary, they would benefit the priveledged at the expense of the poor.
The article cites the following study from The Lancet: Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income countries: a modelling study. “…if routine health care is disrupted and access to food is decreased (as a result of unavoidable shocks, health system collapse, or intentional choices made in responding to the pandemic), the increase in child and maternal deaths will be devastating.” COI: funding by Bill & Melinda Gates Foundation
Related article: Lockdowns will starve people in low-income countries, washingtonpost.com
The Pandemic has Increased Poverty, While Making the Rich Richer
Follow the money.
https://www.dw.com/es/oxfam-la-pandemia-multiplica-pobres-en-a-latina-pero-tambi%C3%A9n-las-fortunas/a-54332114
July 1, 2020
Weird Swedish Data at Worldometer Site
This is a minor unimportant detail. I want to report for thoroughness.


While Europe and Asia Daily Deaths are Decreasing, the Americas are Increasing
Report by Mike Richmond. I'm very upset that it's wrecking my curve-fitting estimate on May 24th.
Update 20200730: This can be automated using OurWorldInData's Data Explorer. There is a slider at the bottom to adjust the dates.
June 28, 2020 Lack of Objectivity, in review
When people get fixated on one way of thinking, they are unable to view data and come to objective results.
Due to lack of full scale testing, the data on the number of cases has been “almost meaningless”. So you have to go by the number of deaths, which at least has a chance of accuracy. 89% of COVID deaths are caused in part by underlying conditions, such as heart disease and cancer, which are the highest ranking causes of death. Time will tell if the CMR crude mortality rate for the entire world goes up significantly due to COVID.
Even if we count all the deaths as just due to COVID, the death rate in the worst affected regions, during the height of the death rate would be around 10 deaths per million per day. Per MILLION. Given the peak death rate doesn't continue, by the end of the year you would have less than one death out of every 1000 persons. Not exactly Black Plague that killed one in three persons in Europe. The following video clip is a historical documentary of the black plague.
People have an instinctual, primordial fear homeostasis. They fear the most miniscule things, because actual things to be afraid of are no longer around in modern society. No lions or hyenas going to hunt you down.
The media, makes money on whatever draws eyes. So they push the pandemic to the fear hungry readers. You can read about how effective a COI is at influencing behavior, here.
The best reason to slow the spread of the virus, is to give the medical field time to learn how to treat the sick. Too often they have been killing patients while trying a therapy that makes their condition worse.
Related articles:
When Will the Madness End, aier.org
La Idiotización de la Sociedad como Estrategia de Dominación, elclubdeloslibrosperdidos.com 201806
June 23, 2020
Infection Fatality Rate
How deadly is the coronavirus? Scientists are close to an answer, nature.com 20200616
This article by Nature magazine is saying that the IFR is 0.6%. I think this will lower in time. People are still in denial, and may overlook a flaw in assessing the data. Remember that some originally said the CFR was 20%. Over time, the scatter plot of claims went down logarithmically.
Update 20200810:
New estimate by CDC reduces COVID-19 death rate to just 0.26% (IFR) from WHO’s 3.4% (CFR), dental-tribune.com 20200524
I found this older article, that is lower than anything I could find on Google when I was searching in June.
The infection fatality rate of COVID-19 inferred from seroprevalence data, medrxiv.org 20200714
“Across 32 different locations, the median infection fatality rate was 0.27% (corrected 0.24%). Most studies were done in pandemic epicenters with high death tolls. Median corrected IFR was 0.10% in locations with COVID-19 population mortality rate less than the global average (<73 deaths per million as of July 12, 2020), 0.27% in locations with 73-500 COVID-19 deaths per million, and 0.90% in locations exceeding 500 COVID-19 deaths per million. Among people <70 years old, infection fatality rates ranged from 0.00% to 0.57% with median of 0.05% across the different locations (corrected median of 0.04%).”
Click Here for the Curious Case of Singapore and Qatar
Related article: Covid-19 vs Influenza, entersingularity.com 20200323
Herd Immunity Threshold
Why herd immunity to COVID-19 is reached much earlier than thought, judithcurry.com 20200510
Herd immunity can be achieved at 43%, new study finds, hindustantimes.com 20200625
The study: A mathematical model reveals the influence of population heterogeneity on herd immunity to SARS-CoV-2, sciencemag.org 20200623
Italy's hard-hit region nears 'herd immunity' as more than half of people tested show coronavirus antibodies, foxnews.com 20200610
Covid-19 immunity could be twice as high as believed, Swedish study finds, telegraph.co.uk 20200630
Herd Immunity May Be Closer Than You Think, wsj.com 20200706
The impact of host resistance on cumulative mortality and the threshold of herd immunity for SARS-CoV-2, medrxiv.org 20200716
Natural herd immunity against Covid-19 could develop from just 10% of the population getting infected — not the 60% predicted from a vaccine, dailymail.co.uk 20200714
” Another new study takes a different approach to estimating differences in susceptibility to Covid-19 and puts the herd immunity threshold even lower. The paper’s 10 authors, who include Gomes and Langwig, estimate that the threshold for naturally acquired herd immunity to Covid-19 could be as low as 20 percent of the population. If that’s the case, the hardest-hit places in the world may be nearing it. “ The Tricky Math of Herd Immunity for Covid-19, wired.com 20200712
June 7, 2020
Containment Does Not Require Lockdown
Kudos to containment, because nobody needs to get another virus. It's like mosquitoes. Sure you can live with them, but if you can wipe them off the face of the earth, then yeah!
Can the virus be eliminated by containment, stopping the virus, before it can spread? Some countries are having success, while others are not. Countries not having success, won't they spread the virus along eventually? Maybe countries practicing containment will have a mandatory COVID test for anyone traveling across their borders, especially from a country known for having COVID-19. Although, countries with a prevalence of COVID-19 will eventually have herd immunity.
I can imagine those recovered from COVID-19 getting passports, and not have to wear a mask, and other liberties. I can imagine some people getting sick on purpose, just to have the liberty afforded by the passport.
The countries having the best success in containing the virus, are practicing compulsory mask wearing, and contact tracing. Including ones that are not having a lockdown. It appears a lockdown is not necessary for containment. It certainly isn't worth the repercussions on society, including psychological damage from isolation, and the financial hardship suffered by the poorest.
The idea that lockdowns are not effective, doesn't make a lot of sense. But consider that there is a human element. I hypothesize that in countries where citizens are used to following strict orders, like China, a lockdown might be effective. Countries where citizens are used to personal freedom are more likely to break rules and seek the company of their close friends, and contagion mostly happens in close quarters. New Survey Suggests 66 Percent of All New Hospitalizations Statewide Are From People Sheltering at Home, ny1.com 20200607
One example where lockdown appears to be effective, is in Iran. It is the only country that had a second wave of daily deaths when emerging from lockdown. More details in the entry for May 9th.
Related article: Do Lockdowns Save Many Lives? In Most Places, the Data Say No, wsj.com I haven't read it due to paywall.
Are There Measurable Effects From a Lockdown Response?
Update 20200728: Related and likely more accurate than measurements of R0 based on cases, is the hospitalizations data covered on July 28.
One reason.com article from June 30, wants to support my case about lockdowns not being effective. ”Did COVID-19 Lockdowns Reach Back in Time to Affect Behavior Before They Were Imposed?“. They present evidence that lockdowns have no noticeable effect on the spread of the virus. See the chart below. Original source of chart, with all the other states ← hover over each state chart to see “shelter started” and “shelter ended”.

My response to this article, is that the chart does not show a sudden drop in R0 after the lockdown day, because not all people take the same amount of time to show symptoms and get tested to be a case.
It's possible that in some states, herd immunity was already taking place before the quarantine lockdown. During the lockdown period, people developed better habits. Then the lockdown was not removed suddenly, but instead a few restrictions were removed with care, making sure not to allow “superspreading” events, like bars and sporting events. This reduced the percentage of the population required for herd immunity, such that R0 has been kept under singularity. Therefore, containment.
Then there's the issue that the value of R0 depends on the change in the number of cases reported over time. Testing capacity has increased over time, so this can make R0 appear to increase, when the actual number of cases is diminishing. This can make R0 itself as useless as the cases data.
Caveats to Modeling R0 Over Time
You can't really compare numbers from one model to another, so in comparing different countries, you have to make sure the same model was used. ”…estimates are very different, and it is probably more useful to look at the trends within each model than to compare reproduction numbers across models.“ preventepidemics.org
Also important to note, is that each country's increase in testing ability over time will artificially increase the measured reproductive number. ”…results are impacted by changes in testing effort, increases and decreases in testing effort will increase and decrease reproduction number estimates respectively (see Methods or our paper for further explanation).“ epiforecasts.io “For example, if numbers of incident infections remain constant but a country begins to find and report a higher proportion of cases, then an increasing value of the reproduction number will be inferred. This is because all changes in the number of cases are attributed to changes in the number of infections resulting from previously reported cases, and are not assumed to be a result of improved testing and surveillance.” welcomeopenresearch.org
Case Counts Are Not Representative of the Pandemic
While death counts are not entirely accurate, they are more accurate than the number of cases reported for COVID-19. Coronavirus Case Counts Are Meaningless, fivethirtyeight.com Confirmed Coronavirus Cases is an 'Almost Meaningless' Metric, bloomberg.com Daily new cases are not an accurate assessment, because not everyone who is infected with COVID gets tested. Governments are ramping up their testing abilities to test more people, so an increase in daily new cases can misrepresent the progression of the pandemic.
Update 20200611: “Sweden announced its highest daily tally of novel coronavirus infections on Thursday, a record 1,474 new cases that authorities said was due to a long-delayed surge in testing.” Coronavirus cases hit daily record in Sweden as tests ramp up, reuters.com
Update 20200616: ”…Prime Minister Stefan Löfven insisted that the situation was improving in Sweden: 'During a period where we have a high number of people being tested, it looks like we have a sudden increase in cases. But the number of people hospitalised for Covid-19 is going down and the number of deaths is going down. So authorities have to start comparing apples with apples, instead of apples and oranges,' he told Swedish Television on Sunday.“ Will Sweden's reputation survive its unique coronavirus response?, thelocal.se
Sweden's Herd Immunity
Given the downward trajectory of daily deaths, Sweden is on its way to accomplishing herd immunity?
The decrease in daily deaths could also be attributed to the previous deaths of those with terminally ill diseases, like cancer and heart disease, who, being hospital mainstays, were exposed and succumbed to the virus. Perhaps there are now less terminally ill for the virus to prey on.
Doctors may also be doing a better job of treating patients in critical condition, where before their efforts were either futile and/or made the patient's condition worse.
Apart from testing for the virus itself, there is antibody testing. Antibody tests may not be accurate, because those already recovered from the virus will gradually cease to produce antibodies, while still being capable of producing them in case of another exposure to SARS-CoV-2. However, current studies are pointing to a likelihood, that the half life for antibody production is long enough to not affect current antibody tests. Then there is also T cell immunity, which does not require antibodies. I think the daily deaths charts are more indicative of the current state of the COVID threat.

June 5, 2020
COVID-19 Immunity Likely to be Long Lasting
Whilst research by the University of Amsterdam is not encouraging regarding CV19 immunity as it suggests antibodies may only protect for 6 months, (Edridge, et al (2020). Human coronavirus reinfection dynamics: lessons for SARS-CoV-2). Other data, however, is suggesting T cell response may provide long term immunity to COVID19 and indeed that T cells from a previous, different coronavirus respiratory virus outbreak in Germany a year or two ago, already gave immunity to many in Germany. See T cells found in COVID-19 patients ‘bode well’ for long-term immunity.
This may explain why some areas of the world are experiencing the pandemic very differently from others. Particularly encouraging in this respect is the fact that T-lymphocyte immunity against the Middle East Respiratory Syndrome coronavirus (MERS), can be detectable for 4 years. See What policy makers need to know about COVID-19 protective immunity.
This interview with the Chair of Oxford University Medical, Professor Sir John Bell, by former UK Secretary of State for Health, Lord Waldegrave is very informative regarding immunity. Sir John is responsible for the Chadox1 vaccine programme in which the US has just invested $1 billion in return for an option on 300 million of the first 1 billion doses. source
Project fear tells us there is no immunity, we will get it repeatedly and we will all die at least twice. Actually the reports of people getting it twice are pretty iffy and not repeated anywhere else. Best studies show 97% get measurable IgG: maybe the other 3 just didn’t quite tickle the threshold. Even if the antibody levels drop over time, experience with other viruses suggests reinfection will boost immunity before getting sick. So I see no evidence to be scared of getting it twice. Those with shares in drug companies and vaccine manufacturers might try and peddle a different story. As always with dramatic headlines “follow the money”. Dick Stockley, doctor, general practitioner
In conclusion, reinfection with SARS-CoV-2 seems unlikely taking into consideration our knowledge on viral neutralizing antibody duration from past respiratory illnesses, the type of specimen collection and technical errors associated with each component of swab testing, the methods used before discharging these patients, the presence of fecal viral RNA without evidence of replication-competent virus in fecal swabs, and finally the reassurance from the animal study. COVID-19 Reinfection: Myth or Truth?, SN Comprehensive Clinical Medicine
Related Article: Coronavirus hopes and fears center on 'immunity', medicalxpress.com
You Maintain Defenses for 10 Billion Types of Pathogens, So Why Do People Think COVID-19 Is Different?
Dedicated to all you Vader Haters
The Virus Wars website reviews that you breathe in over 100,000,000 viruses every day. “Each of us has more than 10 billion different kinds of antibody – that means there are more different antibodies inside you right now than there are people in the world.” You don't think of people as constantly sick and contagious. Why would those immune to COVID become reinfected and contagious? Don't listen to CDC, they value their jobs too highly to educate the public. They would rather say they don't know.
May 24, 2020
Overreporting the Number of Confirmed Cases in USA
It appears the CDC and many states are confounding the number of new cases, by combining positive results from both COVID tests and antibody tests. How Could the CDC Make That Mistake?, the atlantic Someone who has already recovered from COVID, will test positive for antibodies, but that doesn't mean they are a new COVID case, to be reported in statistics for daily new cases.
“The Centers for Disease Control has been lumping together tests for active coronavirus with tests for recovered patients, boosting testing totals but muddying the pandemic’s course.” C.D.C. Test Counting Error Leaves Epidemiologists ‘Really Baffled’,nytimes.com
Click Here for an Exception in Florida
Is the Death Toll Going to be Similar to the Flu?
As the CDC has stated, the high end of a flu year claims the lives of 646K individuals on Earth (between 291,000 and 646,000). How are we doing at the moment with COVID?

If precautionary measures had not been taken, I think the death toll would be greater, but not far beyond 1 million.
Click here for a failed projection
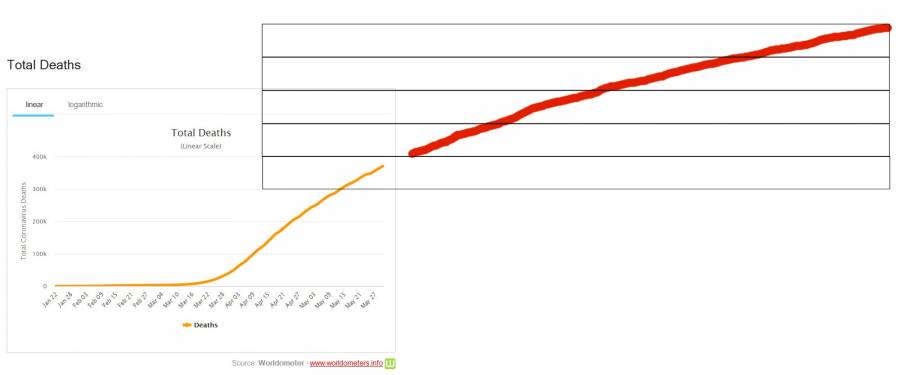
May 13, 2020
Immunity and Antibody Tests
I read statements like: “There is no certainty at the moment that being infected with Covid-19 offers permanent, or even temporary, immunity against the virus.” I really doubted this was true, because how can you recover from infection without antibodies? So I asked a virologist, Liz Kalverda. She said:
You have generic immunity which attacks anything non self as well as learned immunity. It takes quite a while to “train” the lymphocytes. Plus babies don't develop this lymphocytes based immunity till they are about 6 months old. Immunity only applies to b and t cells.
So I asked, what about these super accurate antibody tests coming out?
Feeling annoyed at being asked so many questions, she briskly inserts the genetically engineered coronavirus test tube into the centrifuge, and responds:
Ok, long answer…
Antibodies are part of the learned immunity system. The cells involved in immunity are the memory b cells. Your b cells make antibodies which help to clear viruses (which occurs quite late the first time your body experiences a virus). One b cell can make loads of antibodies, so the antibody levels can raise quite fast without there being that many specific b-cells produced. If you don't make enough memory cells the immunity won't last long (if at all).
If you have a really mild case, which the body gets rid of quickly, it may be too quick to have started making antibodies. If the infection lasts a bit longer you may be producing antibodies, but not have enough memory cells to maintain immunity. Once you have recovered fully from the virus, even if you are immune you won't have antibodies, as they are only produced when exposed to the virus.
This is why if you are unsure if you have been exposed to TB, or if the vaccine has taken, they give you the skin test to see if you have an immune reaction to it, as they can't see the antibodies just in the blood normally.
When you have a vaccine it tends to have adjuvants in, which are there to activate your immune systems so you produce the b cells quicker (although newer vaccines work differently).
Therefore if you have the virus, and have been moderately ill for a few days you will probably have antibodies, but may not have immunity. If you have immunity but have not recently been exposed to the virus you may be immune but not show antibodies. This is why antibody testing may be useful to see if you have the disease, but may not show that you've had it, or are that you are in the early stages of the disease. This is why we haven't been successfully using antibody testing, because it is being used on the wrong population of people.
When I asked Guy Grotke, B.S. Biology & Chemistry, How certain is it, that everyone who gets COVID-19 develops antibodies? Is it possible to get over COVID without antibodies?, he answered:
People could make IgM antibodies but not the longer lasting IgG antibodies. This is call “failure to seroconvert”. A lot of immunologists are concerned about this possibility. You also have an innate immune system that could kill of a very light infection with no antibodies at all.
I'm sure there isn't certainty of just about anything, and we should be aware what possibilities exist. However,
…it looks like SARS-CoV-2 probably induces immunity like other coronaviruses. That means that the human body will probably retain a memory of the virus for at least a few years and should be protected from reinfection, at least in the short-term.
“We do not have any reason to assume that the immune response would be significantly different” from what's seen with other coronaviruses, said Nicolas Vabret, an assistant professor of medicine at the Mount Sinai Icahn School of Medicine who specializes in virology and immunology. livescience.com
Any city or region or country, who instead of having lockdown chose the goal of achieving herd immunity, may serve as a reference. If their daily-cases and daily-deaths is decreasing with time, the downward trajectory would imply that herd immunity is having its effect.
May 10, 2020
Compulsory Face Masks vs Herd Immunity
By the 5th of May, more than 50 countries have made mask wearing compulsory. Austria had a 90% drop in COVID cases two weeks after requiring people to wear face masks. “Czech Republic and Slovakia. As two of the first countries to make masks compulsory in Europe, they now enjoy a small infection rate per capita.”
Most Swedes still do not wear masks: “Many factors would affect the unfolding scene of humankind’s future. But it is not implausible that that scene is better when Swedes mostly do not wear masks on public transportation than when they do.” This is because the Swedish approach is to arrive at herd immunity, where roughly two thirds of the population is immune. “Giesecke argues that the virus is essentially unstoppable, until either herd immunity is reached or an effective vaccine is widely available, perhaps nine to 18 months from now, according to the most hopeful projections. In a letter to the British medical journal Lancet, Giesecke wrote that “everyone will be exposed” and that strict lockdowns only push severe cases into the future.” washingtonpost.com
However, could it be possible to reduce R0 below singularity, such that the contagion extinguishes without reaching its potential percentage of the population? There wouldn't be herd immunity, but it wouldn't matter if the virus were to go extinct. Do we really want to cause the extinction of another of God's creations? (Oh yeah, that's sarcasm) In Denmark, lockdown has been eased and through precautions, R0 has been lowered to 0.9. Technically, R0 decreases with time, the greater the percentage of persons are already immune.
Increases in All-Cause Mortality Can Be Attributed to COVID-19
Since the start of the pandemic, the death counts from COVID-19 may be under-reported. A few data samples show that all-cause mortality (aka Crude Mortality Rate) has increased significantly more than what is being reported for COVID-19: https://www.weforum.org/agenda/2020/05/covid-19-death-toll-misleading-all-cause-mortality-excess-deaths-pandemic. However, considering 89% of persons had underlying conditions, it's possible COVID took out those that would have died later in the year. The Crude Mortality Rate averaged out over the year may give a more approximate death toll estimate for the COVID-19 pandemic.
May 9, 2020
No Significant Increase in COVID-19 after Countries Lifting Lockdown
Iran lifted its lockdown on April 18th, 2020, and represents the worst case of a second wave of infections that I have found. Other countries have a minor or non-existent second wave. Health authorities in Iran ”warned of a second wave of COVID-19 infections“. However, three weeks later, a second wave has not been significant.
Many other countries are easing off their lockdowns without a second wave cnn.comtelegraph.co.uk, including Austria, Switzerland, Germany, Norway, and Denmark. For future reference, you can scan for second waves by country, lookiing at the charts on politico.com or John Hopkins.
Update 20200517: Instead of a second waves ramping up like the first, countries are prepared to take early precautions at the sign of new cases. Instead of waves there will be ripples. China is playing lockdown whack-a-mole in its battle against a second wave of Covid-19 cases, although in regions that did not initially experience an outbreak.
Update 20200605: Iran is having a second wave of COVID-19 cases, but the number of daily deaths has not increased. Maybe they will in another month? Maybe those most susceptible have already succumbed, due to underlying conditions such as cancer and heart disease. Time will tell.
Update 20200622: Unlike the other countries mentioned, Iran is the only one with a second wave in the chart of daily deaths.
Update 20200711:
I think I figured out why COVID is lasting so long in Iran. R0, the basic reproduction number, or how many people one sick person infects, has not been much over 2 in Iran. The transmission rate is low compared to other countries who's entire population was quickly consumed with viral infection. The candle that burns half as bright, burns twice as long. Note there are some caveats to the R0 modeling, but Iran has kept a *level* rate of testing, compared to USA.
This hypothesis is further confirmed by the relatively low number of daily deaths in Iran compared to other countries that had higher peaks:

This phenomena could hint that herd immunity is taking effect, in countries that have experienced initial outbreaks of higher magnitude.
Click Here for the original charts where I first noticed a second wave of cases in Iran


April 28, 2020
Coronavirus Antigenic Drift Less Likely Than Influenza
An explanation of why Coronaviruses are much less likely to mutate successfully, is that the Receptor Binding Site (RBS), which attaches to a receptor on mammal cells, is much larger than for influenza. The RBS must be conserved in a mutation, whereas other parts of the outer shell of the virus can mutate more freely.
Antibodies attach to the outer shell of the virus. With influenza, because the RBS is only a small part of the outer shell, the outer shell can change significantly, necessitating a different antibody to recognize the virus. With coronaviruses, it is more likely that one antibody will cover many strains.
Also, coronaviruses are physically larger than influenza viruses. I hypothesize that the added size brings additional 3 dimensional intricacy, where a random mutation is less likely to be functionally tolerated, resulting in an unviable strain.
Update 20200515: Unlike influenza, coronaviruses have an RNA proofreading mechanism, “which keeps the virus from accumulating mutations that could weaken it … Influenza mutates up to three times more often than coronaviruses do…” nature.com
However, a mutation is still possible, and there is the hope that it does not happen before either a sufficient number of persons have natural immunity, or a vaccine is ready: ” SARS-CoV-2 is new to us … our lack of pre-existing immunity and its high transmissibility relative to influenza … If the pandemic fails to wane, this could exacerbate the potential for antigenic drift and the accumulation of immunologically relevant mutations in the population during the year or more it will take to deliver the first vaccine. Such a scenario is plausible, and by attending to this risk now, we may be able avert missing important evolutionary transitions in the virus that if ignored could ultimately limit the effectiveness of the first vaccines to clinical use. “ biorxiv.org
Update 20200808: There may be a new genetic variant described in the article Discovery and Genomic Characterization of a 382-Nucleotide Deletion in ORF7b and ORF8 during the Early Evolution of SARS-CoV-2, 20200721.
Here, we report a 382-nucleotide (nt) deletion in SARS-CoV-2 that truncates open reading frame 7b (ORF7b) and ORF8, removing the ORF8 transcription regulatory sequence (TRS) and eliminating ORF8 transcription. The earliest 382-nt deletion variant was detected in Singapore on 29 January 2020, with the deletion viruses circulating in the country and accounting for 23.6% (45/191) of SARS-CoV-2 samples screened in this study. SARS-CoV-2 with the same deletion has since been detected in Taiwan, and other ORF7b/8 deletions of various lengths, ranging from 62 nt to 345 nt, have been observed in other geographic locations, including Australia, Bangladesh, and Spain. Mutations or deletions in ORF8 of SARS-CoV have been associated with reduced replicative fitness and virus attenuation. In contrast, the SARS-CoV-2 382-nt deletion viruses showed significantly higher replicative fitness in vitro than the wild type, while no difference was observed in patient viral load, indicating that the deletion variant viruses retained their replicative fitness. A robust antibody response to ORF8 has been observed in SARS-CoV-2 infection, suggesting that the emergence of ORF8 deletions may be due to immune-driven selection and that further deletion variants may emerge during the sustained transmission of SARS-CoV-2 in humans.
I'm not completely sure, but I don't think this represents a completely new antigen, rather, an antigen that is somewhat less susceptible to existing antibodies.
Update 20200921: There are now 3 new variants. The South African version being the most different antigen, capable of infecting a substantial percentage of existing immune individuals.
“A typical SARS-CoV-2 virus accumulates only two single-letter mutations per month in its genome — a rate of change about half that of influenza and one-quarter that of HIV, says Emma Hodcroft, a molecular epidemiologist at the University of Basel, Switzerland.” The coronavirus is mutating — does it matter? nature.com 20200908
April 23, 2020
Effectiveness of Different Precaution Strategies
R0 (Transmissibility) could be further reduced without a lockdown, by everyone wearing a mask. “In Hong Kong, only four confirmed deaths due to COVID-19 have been recorded since the beginning of the pandemic, despite high density, mass transportation, and proximity to Wuhan. Hong Kong’s health authorities credit their citizens’ near-universal mask-wearing as a key factor” The Atlantic, April 22nd However, the drastically different death tally could be because measures were taken early, well before other countries, or may have a yet unknown explanation. Additional sources: contagionlive.com qz.com
Compare to the Swedish approach, of only sanitizing, hand washing, and social distancing. Could they have been mistaken in their belief that facial coverings are not effective? Or, perhaps they see this virus as not apocalyptical, and don't think it warrants that specific change in lifestyle. Refer to the entry below about Objectivity.
Update 20200502: Sweden is fairing comparably to countries that are observing quarantine and obligatory mask wearing. As can be seen below, their daily death rate is already decreasing. Click here to see a comparison between countries, of the number, per million, of daily deaths. Sweden deaths per capita per day have stayed below those of Belgium, Ireland, United Kingdom, Italy, Spain, and France.

Update 20200505: Belarus, with no social distancing measures, is doing better than other countries in its vicinity, having a very low death rate per capita. Compared to Sweden and Belarus, countries with higher mortality rates have a higher population density. Sweden 22 per km2. Belarus 47 per Km2. Italy 206. Belgium 383. Spain 91. France 122. UK 281. Ireland 72. The plot below of deaths-per-capita vs population-density for a large number of countries does not show any trend. However, urban vs rural distribution is not considered, and neither is the number of days since a quantifiable contagion.
Update 20200515: ” There is no correlation between fatalities and lockdown stringency. The most stringent lockdowns – as in China, Italy, Spain, New Zealand and Britain – have yielded both high and low deaths per million. Hi-tech has apparently “worked” in South Korea, but so has no-tech in Sweden. Sweden’s 319 deaths per million is far ahead of locked-down Norway’s 40 and Denmark’s 91, but it’s well behind locked-down UK’s 465 and Spain’s 569. “ theguardian.com

April 20, 2020
Earlier Precautions Fare Better in Reducing Contagion
COVID is different from other viruses in that the sick do not show symptoms in the first 2 to 14 days, with an average of 5 days. Although being asymptomatic during this period, they are contagious. This makes containment difficult, if you are only trying to isolate those showing symptoms.
The countries / cities that fared the best are those whose citizens had advance warning, and took precautions to reduce contagion, early, before a large number of cases took effect. Below a model showing a possible effect of waiting one day:

April 19, 2020
Comparing COVID-19 to the Hong Kong Flu
This article was updated 20200511, with the availability of preliminary data to make at least an educated guess possible.
Previously, I compared COVID to swine flu, but COVID likely has a higher R0 (transmissibility aka "basic reproduction number") and a higher mortality rate. So looking back on the timeline, for a disease with a higher kill rate, is the Hong Kong Flu of 1968.
The mortality rate of the Hong Kong Flu is not given the same metric as is given in the media for COVID. It is given a crude mortality rate (CMR), which is the number of deaths per 100K population per year. Scientists measure the increase in mortality of the entire population from all causes during the pandemic, instead of giving a ratio of deaths to cases of flu. The increase in the mortality rate of the entire population during the Hong Kong Flu was 0.017%, or an additional 16.9 dead per 100K per year. Over three years this amounted to between 500K and two million deaths.
For COVID-19, tons of sites incorrectly give the Case Fatality Rate (CFR), while calling it the Crude Mortality Rate. Lies! That would send the total death toll through the roof. The asymptomatic, and those that the virus never infects are excluded.
Let's say that COVID has a similar CMR to Hong Kong Flu. The population of the earth is 7.8 billion, so in a year the number of dead from COVID would be 1.32 million.
Update 20200511, deleted because Belgium is overestimating deaths: An estimation for COVID's Crude Mortality Rate can be extrapolated from John Hopkins Data on deaths per 100K population. Belgium is the worse off, at 75 deaths per 100K. Let's make a conservative estimate that they reach 90 per 100K by the end of the pandemic, and that eventually, the rest of the world will be as bad as Belgium. That would mean 7 million deaths.
For Hong Kong Flu, the “Estimates of the basic reproduction number (R0) were in the range of 1.06–2.06 for the first wave and, assuming cross-protection, 1.21–3.58 in the second.” nih.gov
Update 20200511:
COVID has an unquarantined R0 of 3.86, and a Symptomatic Case Fatality Rate of 1.3%. The SCFR is from USA data, so we have to round down for a world average, considering USA contains more unhealthy people. Let's estimate 1%.
A large percentage of persons infected with COVID-19 are asymptomatic. Studies show figures of 78%, 96%, and 88%. If we estimate that 80% of the population that is infected with COVID never experience symptoms, then the IFR Infection Fatality Rate is 0.2%, or four times as much as influenza's worst case of 0.05%.
Assuming the virus reached 1-1/R0, or 74% of the population before herd immunity took effect: 7.8 billion x 0.74 x 0.02 = 11.5 million deaths.
Update 20200804:
” Another new study takes a different approach to estimating differences in susceptibility to Covid-19 and puts the herd immunity threshold even lower. The paper’s 10 authors, who include Gomes and Langwig, estimate that the threshold for naturally acquired herd immunity to Covid-19 could be as low as 20 percent of the population. If that’s the case, the hardest-hit places in the world may be nearing it. “ The Tricky Math of Herd Immunity for Covid-19, wired.com 20200712
7.8 billion x 0.20 x 0.02 = 3.12 million deaths. This still doesn't seem right to me. The most extreme low prediction:
7.8 billion x 0.10 x 0.02 = 1.56 million deaths.
In order to make a direct comparison with the Hong Kong Flu, we must calculate the Crude Mortality Rate for COVID-19. Let's consider that all the deaths took place in one year (considering the high transmission rate, and projecting only one viral wave). The global death rate from all causes is estimated to be 7.7 per 1000, or 7700 per 100K population, adding up to 60 million deaths per year for 2020. Thus, the estimated increase in CMR is (1.56/7800) ⇒ 0.020% for COVID-19, higher than the 0.017% for the Hong Kong Flu.
Possible Long Term Changes in Socialization
The R0 can be lowered dramatically by practicing precautions, and may make the difference in reducing deaths by millions. Update 20200511: In Denmark, lockdown has been eased and through precautions the R0 has been lowered to 0.9, and if kept at that rate, the virus would extinguish before herd immunity was reached.
Perhaps everyone will be wearing mouth coverings in the future? Social dancing may have a new look, as all will be adorned in hijab. Or perhaps a better treatment will be found for COVID, or the number of daily deaths will be low enough to appease the news media gods, and things will return to “normal” until the next pandemic.
April 18, 2020 Lack of Objectivity

SARS-COV-2 is not the Only Game in Town
It's good to think in many dimensions. Instead of only trying to keep people safe from COVID, let's make a better world overall. We've been ignoring many of the world's problems, and we go about this in our normal lives. Why is COVID now something urgent, when there's been urgent everywhere around us?
While diseases are not something we have complete control over, there are self-inflicted deaths that we are ignoring. Let's take a long hard look at “normal”. For comparison, the CDC states that globally, there are 1.35 million vehicular accidents every year. Does the population freak out about the risk, like it has with COVID-19? Hardly. The topic doesn't get that level of sensationalist mass media. People will drive to Starbucks for a coffee, just to get out of the house. Somehow, people have lost objectivity, that there is an equal chance of dying from a car accident compared to a viral infection.
In Los Angeles, the quarantine has reduced auto accidents by half, which should help free up hospital beds. ER doctors in some regions are unemployed as hospitals become sedentary. “The reductions in air pollution in China caused by this economic disruption likely saved twenty times more lives in China than have currently been lost due to infection with the virus in that country.” cnn.com “China remains the world’s deadliest country for outdoor air pollution, which kills more than one million people a year.” nature.com
CDC states that “between 291,000 and 646,000 people worldwide die from seasonal influenza-related respiratory illnesses each year, higher than a previous estimate of 250,000 to 500,000 and based on a robust, multinational survey”.
Click here for a vouch of confidence in the CDC
COVID is not like flu, because you can be contagious without first showing symptoms. Additionally, COVID is more contagious than the flu, spreading more easily. I can understand that people are afraid, where in some areas, COVID will be the number one cause of death for many weeks. If COVID ends up killing the same amount of people as flu in a year, it would just have done so more quickly. COVID would burn the timber in a few months, while the flu would keep us warm all year.
By itself, COVID may not be a bad threat, but when it reaches those who already have disease, it makes for deadly cases. Usually, the causes for the highest crude mortality rates are cancer and heart disease. Who is COVID killing? Cancer, heart disease, and diabetes patients. Underlying conditions in general, at a ratio of 89%. Not many healthy people die from COVID-19, no matter how many dramatic stories of a young person dying you may see on the news. When someone is listed as having died from COVID, you may not have the full picture:

![]()

Think You Have COVID? Don't Go to the Hospital
If you go to the hospital, chances are you will get more cooties. If you have the flu, you may catch COVID, or if you have COVID, you may also catch the flu. Season with a little pneumonia. A recipe for a very bad case. One shouldn't blame all the deaths exclusively on the COVID virus. COVID-19 is adding another front to the attack.
So maybe, while your immune system is under attack, it's a good idea to stay out of the hospital, far away from other diseases. Doesn't that just make sense? Does Going Into Hospital Make You Sick? talks about hospital readmission rates. Cancer patients are contracting COVID at an alarming rate.
In France they used to have mobile doctors, before funding cuts left the health care system barely ready to handle any new challenge.
What I'm trying to say here, is that social normalcy is barbaric, and people are in denial of that fact because of an inherent need to think otherwise. An inherent need to live in a fairy tale where they are not actively involved in supporting barbaric practices.
Instead of shooting yourself in the foot, why not focus instead on making the world a better place? We are laying waste to the planet, and we need to change our lifestyles drastically. Instead, we have lockdown because of a stupid virus? Yes it's great that we may wear masks to protect others, but to spend so much energy and attention on just that? Having an intelligent conversation is difficult when reality is politically incorrect. If you are not connected to reality, you will follow the news media mob.
The same crowd following the media mob, will also check in to the local hospital to be treated by “experts”. Because a conformist has a need to trust experts, and likely doesn't spend time reading that experts are clueless about how to treat COVID. In NYC, medical mismanagement and negligence is competing with COVID to see who can kill more patients: dailymail.co.uknypost.com.
Thus the conformist will get in a car to go to the hospital, needlessly increasing the risk of death for everyone while adding more pollution. For a conformist, that's normal, and trying to talk reason into them is like trying to strip away their security blanket.
Sensationalist Media Feeding the Drama Seekers
COVID is bad, but we are only paying attention to it, because the media has focused on it. COVID is sensationalized. They had spread the gospel that the risk of having a severe case, where you require a respirator, is 20%. The 20% figure is incorrect, but people seem to have a primordial need for something to be afraid of, so it stuck. COVID is the shiny new threat to be afraid of.
Covid is the shiny new threat to be afraid of.
Iceland tested a larger percentage of their population than any other country, for active COVID-19 infections. Although not randomly, because people afraid of having COVID were more likely to go and be tested. Of those arriving on open invitation, half affected by COVID had no symptoms, which means that likely, even more carriers without symptoms didn't bother to get tested. They did not follow up with the asymptomatic carriers to find out if they developed symptoms.
The New York-Presbyterian/Columbia University Irving Medical Center, published a study from their labor and delivery unit. 88% of the women that were positive for COVID were asymptomatic. Granted, it's a young segment of the population.
Let's go on a whim, and say that in the general population, only one in four develop symptoms. They are or were at some point, silent carriers. None of them are counted towards the percentage of cases requiring a respirator. Let's say that half of people who develop symptoms actually go to the hospital. There's the bunch like me that get sick and don't go to the hospital, so they don't get counted. That makes one in eight covid cases. In NYC, there are those that go to the hospital and get turned away because they don't have a fever, like my roommate. They are told that because they don't have a fever, they don't have the virus, which is completely bogus. That leaves one in sixteen covid cases.
Back to the 20% figure, that the media has been terrifying people with. If 20% of the 1/16th COVID cases at the hospital end up needing a respirator, you are now at one in eighty cases that require a respirator. There has been many estimates for the Case Fatality Rate, ranging from 1% to 5%. Let's take 3%, and divide this by 16 for our guess of an IFR Infection Fatality Rate: 0.19%.
So the ones that stay in the hospital could be thought of as having a mild case of COVID that the body is fighting off with a fever. They are ok, but they have a weakened immune system. Chances are, they will catch whatever else is going around, and get really really sick. Going to the hospital increases the chance severe illness and chance of death. Can you see how the chance of dying from COVID would be both overblown and self inflicted?
People are suffering by other means as well, not just from this COVID virus. So please, if you want to be a humanitarian, look at the big picture and stop being a drama-seeker. Drama seekers are just as responsible as mass media in spreading misinformation. Instead, research the facts and draw your own conclusions, without fearful emotions or political affiliations clouding your judgement, and be open to change. Make the world a better place.

Government For the People Through Positive Reinforcement
Most politicians want to ride this wave, where they can be seen as taking command of the situation. It's very fashionable right now to protect against COVID. Fashionable to have a police state.
Not all countries are taking freedom away from its citizens. For example, Swedish Prime Minister Stefan Löfven made the following statement: “Us adults need to be exactly that: adults. Not spread panic or rumours. No one is alone in this crisis, but each person carries a heavy responsibility”. click for more about this decision
If you want to raise a child to be a responsible adult, you must treat them as capable of handling responsibility. Sometimes this involves risk. If you want to have a nation of responsible adults, you will have to give them the freedom to make mistakes. Think of God and free will. “The Swedish model of collective action also has important lessons that go far beyond public health efforts.” What Sweden Can Teach Us About Coronavirus, politico.com
Many will want to take away the freedom of the individual to leave their house, because of the potential that this individual could spread or contract the virus, affecting others in time. What holds more value? Safety, or freedom? People have different value systems. I want the individual to have freedom, and the education to take care of themselves and others.
Back to Normal
Based on the projected schedule for Wuhan, China, one could estimate a cycle of 3 to 4 months before precautions are lifted, and civilization mostly goes back to normal. For NYC, that could be the end of May. However, NYC is not Sweden or Iceland. Nor does it have a quarantine that is as strict as China's.
Conflict of Interest Statement
I don't care if we continue to stay locked down or not. I could care less if we continue to stay locked down indefinitely. However, my opinion is that based on the facts, I don't think it's necessary. I think mask wearing, and good hygiene practices, is the key to reducing R0 to less than singularity. I think it is up to any particular country or region to decide if they want to make mask wearing compulsory, or work towards herd immunity.
If anyone hasn't gotten my point yet, it's that there are much more important matters to focus on besides COVID-19, including the corruption of society towards an unsustainable and unhappy future. If you see humor within this rather serious article, it's because I need it. I've tried to uncover as much of reality as possible, in order to educate myself and others. We have nothing to fear, but fear itself. Fear is keeping us from being objective. Fear is keeping us locked down, and fear is keeping us from changing towards a better future.
For those who are using COVID-19 as a means to an end, as in, politically, to actuate changes they think are important, I say that the ends don't justify the means. Honesty and integrity. Humility and equality.
April 13, 2020
COVID-19 Comparison to Swine Flu
This article was not updated with more accurate information that came in the following month.
The large Infograph comparing historical pandemics, shows Swine Flu having 200K deaths. In actuality, Swine Flu likely caused around 300K deaths, with a range from 150K to 580K.
Is Coronavirus more contagious than Swine Flu? It depends on when the R0 (contagiousness or transmissibility) measurement was taken. In Wuhan without containment, the R0 is estimated to be around 3.86. After lockdown, R0 fell dramatically.
The following chart from a Nature article compares the R0 of historical contagious diseases. Swine Flu of 2009 had an estimated R0 between 1.4 and 1.6, with an Infection Fatality Rate of 0.026%.
Compared to other viruses, someone with COVID is contagious in the first few days, without showing any symptoms. This makes quarantine much more difficult. Where the sick are isolated at the onset of both symptoms and contagiousness, R0 is dramatically reduced.
A different metric for viruses is the Case Fatality Rate. Update 20200414: The fatality rate for COVID is 0.5% best measured in the country whose testing has had the broadest reach: Iceland. This is quite different from the 20% CFR mass media was shamefully broadcasting. Another lie.

Do they actually know how many people have contracted coronavirus? No, they don't. They don't test everyone. In the USA, they turn away people that don't have a fever, then have the nerve to say that most people that get coronavirus get a fever. “Iceland lab's testing suggests 50% of coronavirus cases have no symptoms” https://www.cnn.com/2020/04/01/europe/iceland-testing-coronavirus-intl/index.html
The difference that stands out, is that many hospitals are overrun compared to the time of the swine flu. See https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6669026 and http://www.cidrap.umn.edu/news-perspective/2009/05/worried-well-overload-gives-taste-pandemic-scenario But how much of that may be attributed to cuts in hospital readiness, after cuts in funding or privatization? It should not be overlooked that hospitals are affected worldwide.
Hospitals Run Near Capacity
When they say that hospitals are overrun, what exactly does that mean? CNN covered a hospital in Brooklyn, one of the hardest hit. The hospital has a 300 bed capacity, and 100 beds were filled with coronavirus patients. So it seems it doesn't take much to overrun a hospital. They are usually running near capacity.
Click here for a failed projection

sociology/epidemiology.txt · Last modified: 2025/01/05 07:20 by marcos
Except where otherwise noted, content on this wiki is licensed under the following license: CC Attribution-Share Alike 4.0 International

Discussion